Acute Rhinosinusitis (ARS)
-
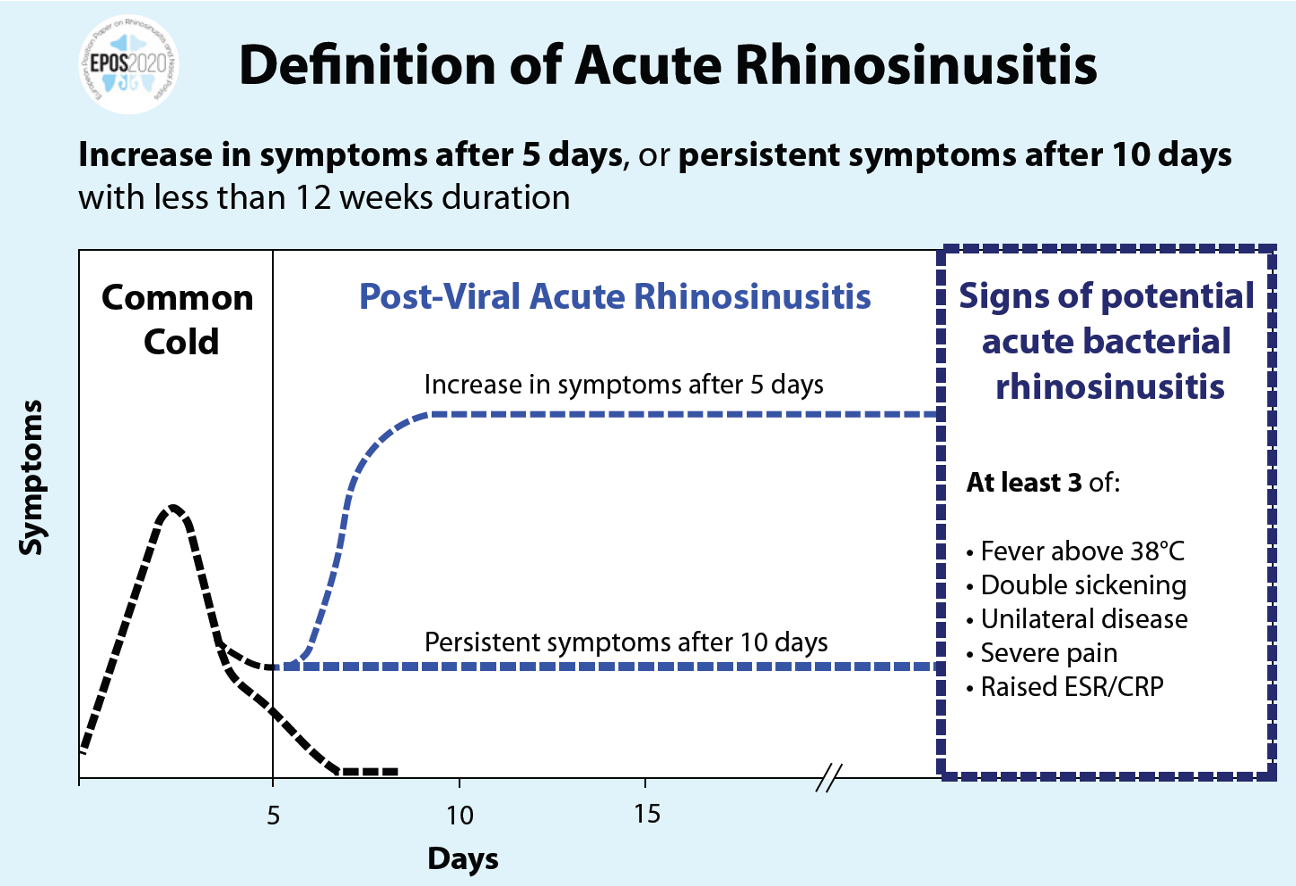
- Symptoms present for less than 10 days and not worsening.
-
Acute Bacterial Rhinosinusitis
- Symptoms fail to improve within 10 days or worsen after initial improvement (double worsening).
-
- Symptoms lasting 12 weeks or longer with inflammation documented by clinical findings.
-
Recurrent Acute Rhinosinusitis
- Four or more episodes per year of ABRS without symptoms between episodes.
Z OSPE
 after 1 month, chronic or allergic most probably
after 1 month, chronic or allergic most probably
Major: nasal discharge, obstruction, anosmia, facial pain minor: dental pain, hyposomnia, headache
Functional Endoscopic Sinus Surgery (FESS)
Steps:
- Medialize middle turbinate.
- Excise uncinate process.
- Anterior and posterior ethmoidectomies.
- Sphenoidotomy.
- Frontal recess dissection.
- Create maxillary antrostomy.
Indications for Endoscopic Sinus Surgery
- Chronic sinusitis,
- Complicated sinusitis,
- Recurrent acute sinusitis,
- Failed medical management of acute sinusitis,
- Fungal sinusitis
- Obstructive nasal polyposis
- Sinus mucoceles
- Remove foreign bodies
- Tumor excision,
- Transsphenoidal hypophysectomy
- Orbital decompression,
- Dacryocystorhinotomy,
- Orbital nerve decompression,
- Grave’s ophthalmopathy
- Choanal atresia repair
- CSF leak repair
- Control epistaxis
- Septoplasty,
- Turbinectomy
Goals of FESS
- Complete removal of all disease.
- Permanent drainage and ventilation of affected sinuses.
- Postoperative access to previously diseased areas.
-20250113111258880.webp)
FESS Orbital Complications
-
Blindness: Indirect injury (retrobulbar hematoma) or direct injury to the optic nerve.
-
Orbital fat penetration: Increases risk of retrobulbar hematoma. Rx: recognize orbital fat (orbital fat floats); avoid further trauma; may complete the FESS; avoid tight nasal packing; Observe for vision changes, proptosis, or restricted ocular gaze
-
Diplopia: Orbital muscle injury.
orbital muscle injury, most commonly from medial rectus and superior oblique muscles -
Epiphora: Injury to lacrimal duct system.
injury to lacrimal duct system, avoid operating anterior to the attachment of the uncinate; Rx: observation initially, if no resolution then dacryocystorhinostomy