(Cerebellar walking & tandem gait)
The cerebellar examination is performed in patients with neurological signs or symptoms of cerebellar pathology, for example: dizziness, loss of balance, or poor co-ordination. There are many causes of cerebellar dysfunction and include vascular, for example: stroke, space-occupying lesions, multiple sclerosis, and genetic conditions such as Friedreich’s Ataxia. The cerebellar examination needs to reflect these symptoms and as such involves examining the gait, balance and co-ordination.

Tandem gait: The examiner asks the patient to walk in a straight line with the heel of the leading foot touching the toes of the lagging foot as if walking on a tightrope. Romberg’s test. Ask the patient to stand with their feet apart and then close their eyes. Any swaying may be suggestive of a posterior column pathology.

- tandem walking - uncover unobvious ataxic gait
- inability to heel walk; corticospinal weakness
- difficulty hopping; weakness, lack of position sense, or cerebellar dysfunction
- difficulty with shallow knee bend; proximal weakness. weak quads, or both
- difficulty rising from sitting position or stepping up on sturdy stool;proximal weakness involving pelvic girdle & legs
- Ataxic gait; lacks coordination, “reeling” with instability, Usually indicates cerebellar disease, loss of position sense or intoxication
Other Signs
- Walk across room, turn and walk back
- Heel & toe walking
- Hop in place
- Shallow knee bend
- Rising from sitting position or stepping up on stool
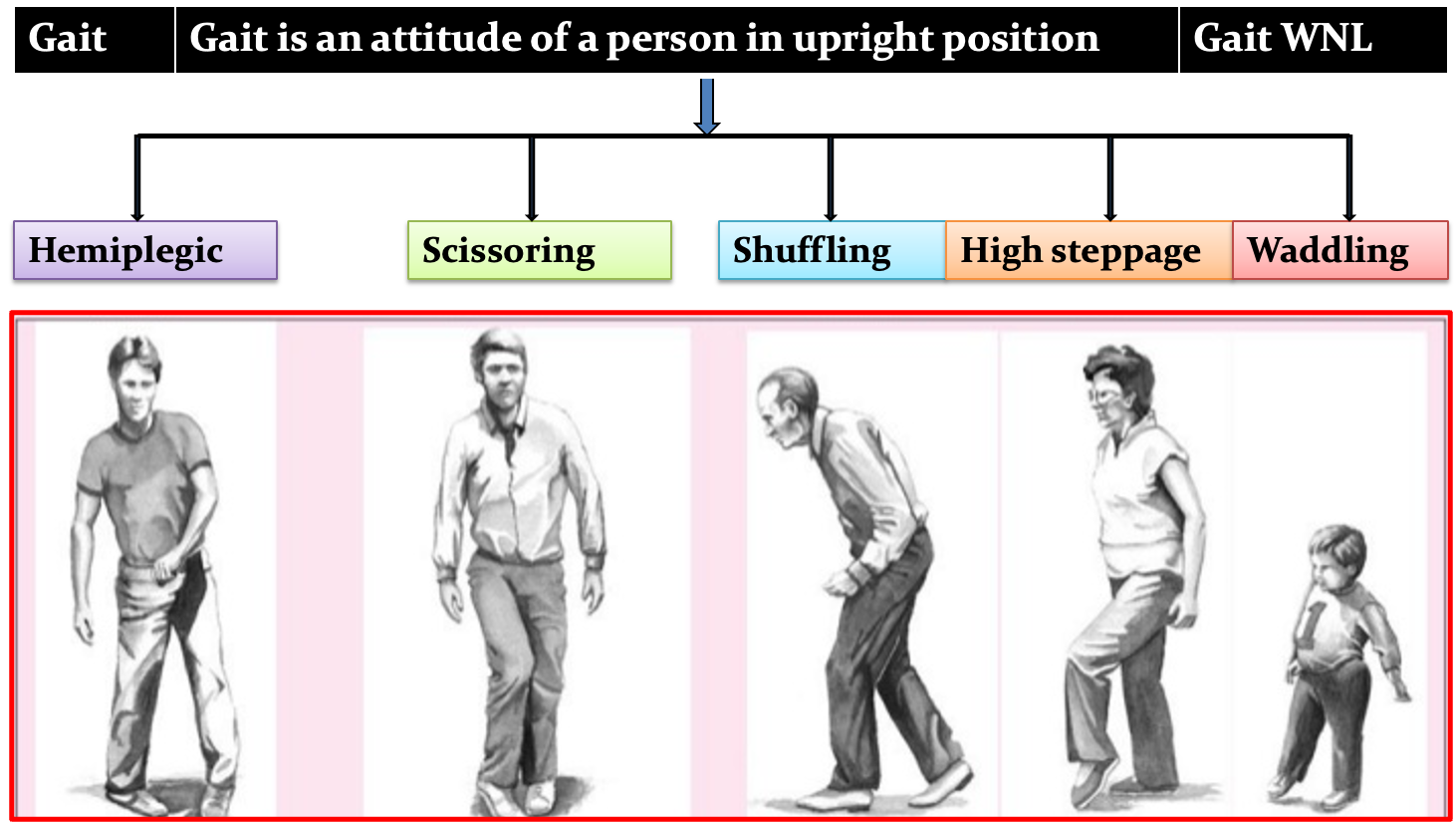
Human gait is defined as bipedal, biphasic forward propulsion of center of gravity of the human body, in which there are alternate sinuous movements of different segments of the body with least expenditure of energy
Types includes Hemiplegic, Scissoring, Shuffling, High Steppage, and Waddling
Y
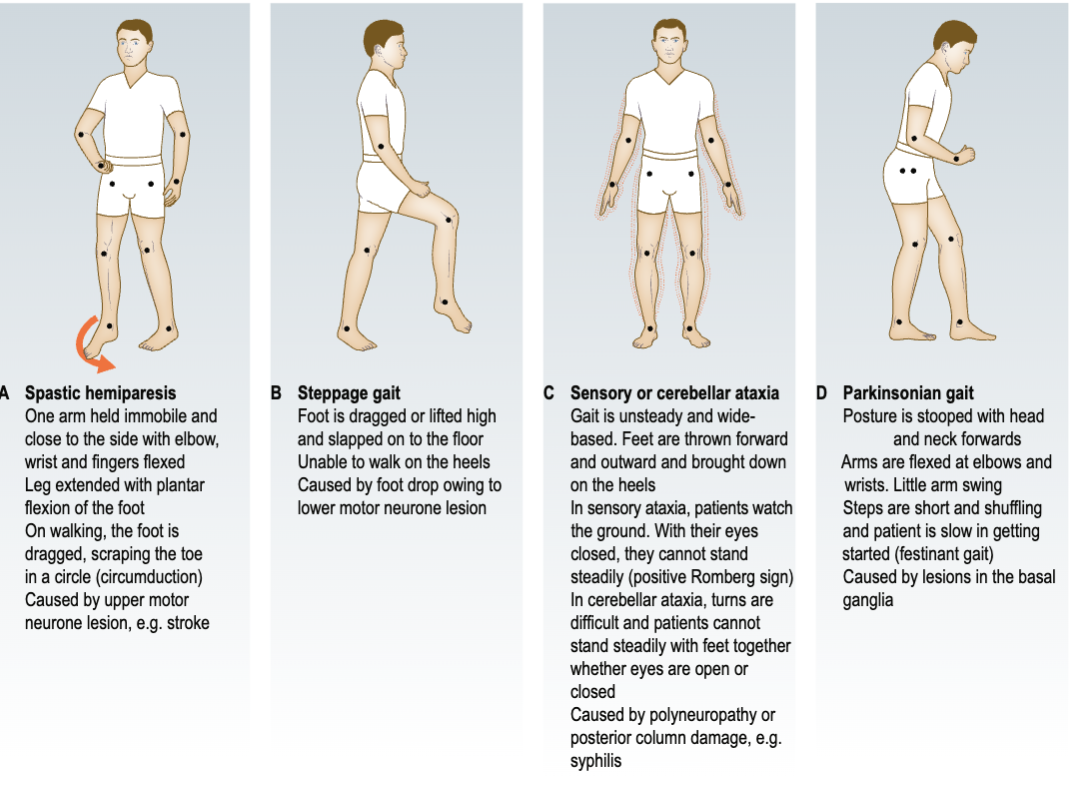
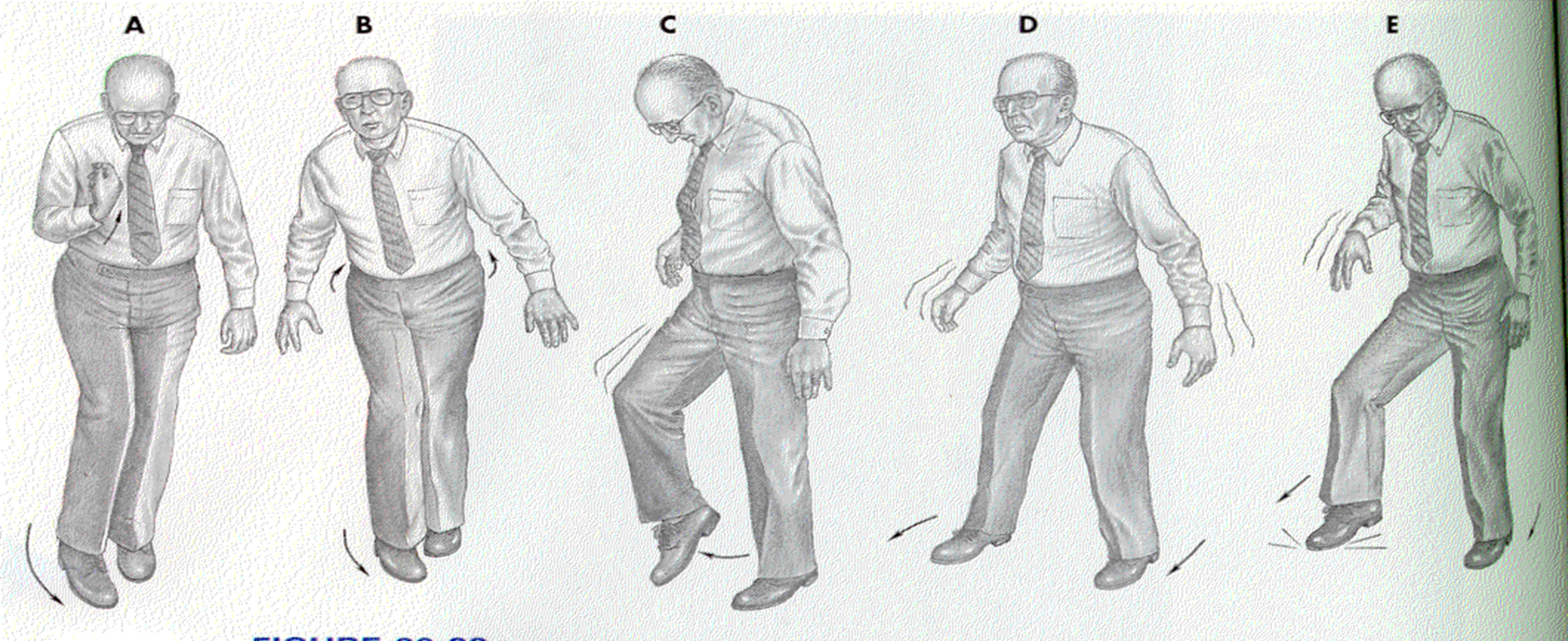 A = Spastic Hemiparesis - the affected leg is stiff and extended with plantar flexion of the foot. Movement of the foort results from pelvis tiliting upward on the involved side. The foot is dragged, often with scraping of the toe, or is circled stiffly outward and forward (circumduction). The affected arm remains flexed and adducted and does not swing.
A = Spastic Hemiparesis - the affected leg is stiff and extended with plantar flexion of the foot. Movement of the foort results from pelvis tiliting upward on the involved side. The foot is dragged, often with scraping of the toe, or is circled stiffly outward and forward (circumduction). The affected arm remains flexed and adducted and does not swing.
B = Spastic Diplegia (scissoring) - scissor gait - patient uses short steps, dragging the ball of the foot across the floor. The legs are extended and thighs tend to cross forward on each other at each step, due to injury to the pyramidal system.
C = Steppage gait - the hip and knee are elevated excessively high to lift the foot off the ground. The foot is brought down to the floor with a slap. The patient is unable to walk on the heels.
D = Cerebellar ataxia - the aptient’s feet are wide-based and there is staggering and lurching from side-to-side - often accompanied by swaying of the trunk.
E = Sensory ataxia - here the patient’s gait is also wide-based. The feet are thrown forward and outward. The foot is brought down on the heel first, then on the toes. The patient watches the ground to guide his/her footsteps. A positive Romberg sign is also present in this gait.