Causes
-
Potassium Shifts from the ICF to the ECF
- Metabolic acidosis
- Strenuous exercise
- Insulin deficiency
- Hyperglycemia
-
Medications
- Potassium-sparing diuretics (spironolactone)
- Potassium supplements (e.g., potassium chloride)
- ACE inhibitors
- Chemotherapeutic agents
-
Impaired Renal Potassium Excretion
- Renal failure
- Renal tubular acidosis (RTA)
- Adrenal insufficiency
- Congenital adrenal hyperplasia (CAH)
-
Movement of Potassium Out of Cells During or After Specimen Collection (Pseudohyperkalemia)
- Hemolysis
- Tumor lysis syndrome
Hyperkalemia
- Serum K+ > 5.5 mEq/L
- Mild: S K+ = 5.5-6.5 mEq/L
- Moderate: S K+ = 6.5-8.00 mEq/L
- Severe: S K+ >8 mEq/L
Lab Tests
- Chemistry for other electrolytes
- Glucose level
- Urinalysis, urine potassium, and creatinine
- ECG
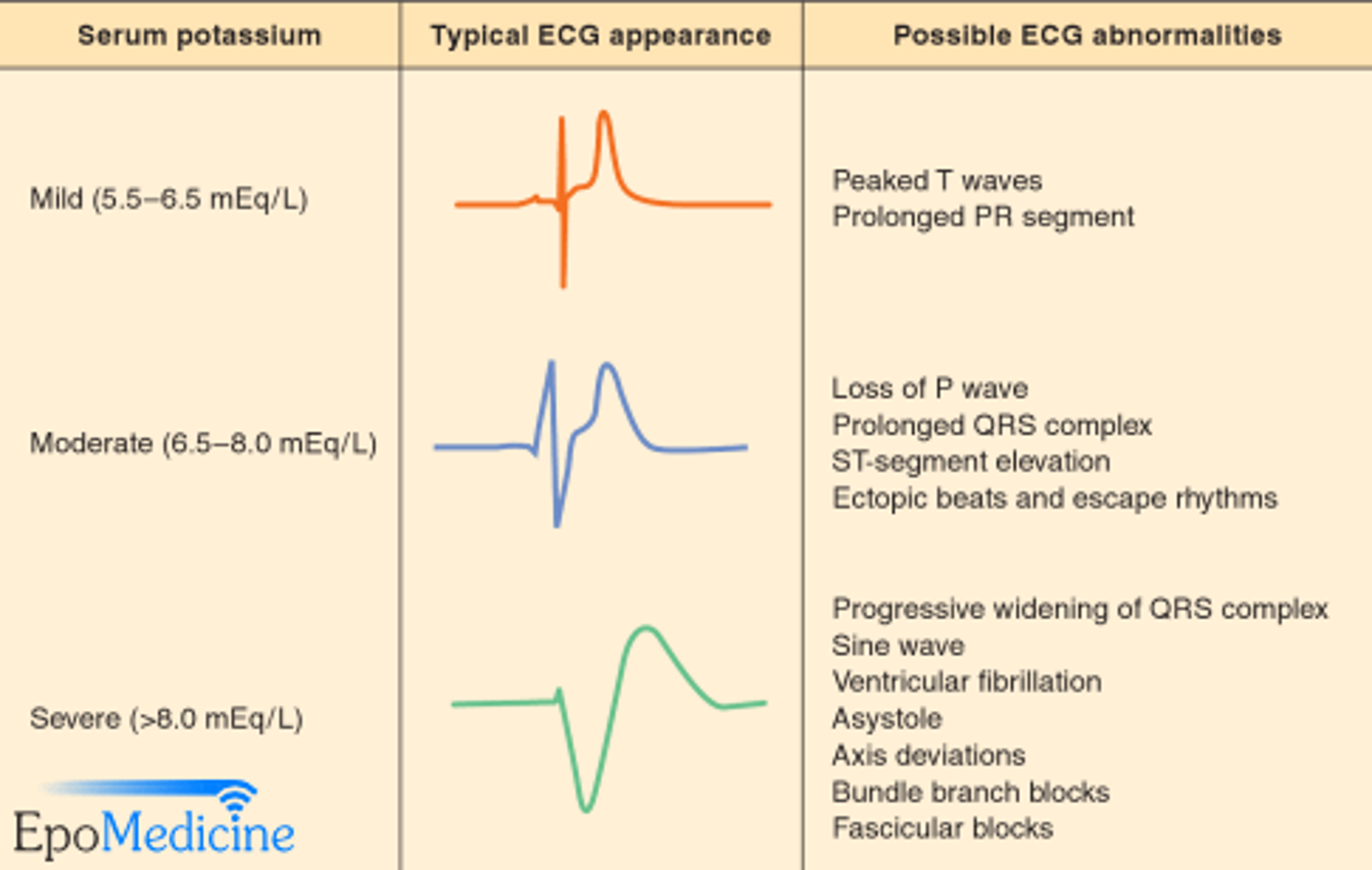
ECG Changes
- Prolonged PR interval
- Peaked T wave
- Wide QRS complex
- Absent P; flattening
- Asystole, VF
Clinical Features
- Muscle weakness, decreased deep tendon reflexes, ileus, tingling of the mouth and extremities, malaise, and tetany.
Hyperkalemia Treatment
First Line
- Salbutamol nebulization: Shifts K into the cells. Effect appears within 20-30 minutes.
Second Line
- Insulin and Glucose infusion: Shifts K into cells. Effect appears within 10-20 minutes.
Third Line
- Furosemide: Excretes K through renal tubules. Effect appears within 60-120 minutes.
- Calcium Gluconate: Given in moderate to severe hyperkalemia to stabilize cardiac conduction.Z (ECG CHANGES GIVE IMMEDIATLY)
- Calcium Resonium (Kayexalate): Antagonizes K effect. Effect appears within 60-120 minutes.Z (PROTECT HEART AND ORGANS AGAINST K EFFECT)