HX
- Abdominal Pain HX
- Biliary colic HX
EX
- Abdomen exam, EX
- Liver mass EX
- Neck mass exam EX
- Peripheral vascular diseases EX
- Breast Lump EX
- Diabetic foot
SK
- Scrubbing & wound stiches SK
- Urehtral Cath - SK
- Nasogastric tube insertion SK
- Digital rectal exam & protoscopy SK
collected from Abdullah Bohairi & Faisal Alkharji
اللهم يا معلّم موسى علّمني، ويا مفهم سليمان فهّمني، ويا مؤتي لقمان الحكمة وفصل الخطاب آتني الحكمة وفصل الخطاب اللهم اجعل ألستنا عامرة بذكرك، وقلوبنا بخشيتك، وأسرارنا بطاعتك، إنك على كل شيء قدير، حسبنا الله ونعم الوكيل
if there are any correction, changes, or addition in your notes please send me message dr.alkharji@proton.me
History Taking:
| Action* | Mark | Given marks |
|---|---|---|
| Self-introduction / greeting and manners | 0.5 | |
| Patient’s personal data | 0.5 | |
| Chief complaint(s) | 0.5 | |
| History of present illness | 0.5 | |
| Relevant systemic inquiry | 0.5 | |
| Past medical/ Surgical history | 0.5 | |
| History of medications/ allergy | 0.5 | |
| Family/social history | 0.5 |
Examination
| Action* | Mark | Given marks |
|---|---|---|
| Permission for examination & explaining procedures | 0.5 | |
| Patient positioning & adequate exposer | 0.5 | |
| Performing relevant examination in proper order | 0.5 | |
| Performing examination using correct technique | 1 | |
| Describing correct physical findings | 1 |
Management Plan
| Action* | Mark | Given marks |
|---|---|---|
| Most likely diagnosis | 0.5 | |
| Differential diagnosis and justify diagnosis | 0.5 | |
| Appropriate investigation request | 1 | |
| Suggest a treatment plan | 0.5 | |
| Total marks scored | ||
| . |
.
.
.
.
.
CCTD History
Abdominal pain/Liver mass, Jaundice, Biliary Colic
Framework
- Demographics (Name, Age, Gender, Nationality, Martial, Residency)
- Chief of complaint (Cause of hospitalization + days)
- HOPI (OPERATES NON PAIN | SOCRATES PAIN)
- B-Symptoms
- Systemic Review
- Past history (medical, surgical, medication, allergies, family, social)
- summary
- differential + justify differential
- investigations - appropriate
- treatment - suggestive
Introduction, explain, Permission, Assure privacy, chap.
Greetings im Mohammed 5th year medical student; could you tell me your name..“amm ahmad”. im here to take your full history, may i proceed? =-
call nurse, assure privacy.
1) Demographics
32 year old Egyptian engineer man married with two kids, lives in Riyadh
In biliary colic presentation in demographics are
- 35 years old male
-
40 age & Females most commonly due estrogen
2) Chief of Complaint
why did you come to hospital; write same as “Abdominal pain ((not specific to Epigastric pain))
- Halitosis
- Abdominal Pain
- Steatorrhoea
- Vomiting & weight loss
- Other Git Symptoms - Constipation, Dysphagia, Acute Diarrhea etc..
- Heart Burn
- GI tract diseases
- Drugs and alcohol
- Functional
- Psychogenic
5 day abdominal pain
Biliary colic presentation example complain pain 5D in right upper quadrant - associated with jaundice
Jaundice Presentation 5D yellow eyes - usually follows through OPERATES METHOD
Ask when the patient first noticed, or someone that noticed since when… without character of pain or site more emphasis on PROGRESSION, TIMING, & EPISODE
3) HOPI
5 day progressive stabbing abdominal pain located on epigastric region radiating to the back increased with movement, subsides with rest prominent in the morning subsides later in the day… associated with vomiting & constipation, no diarrhea flatus or B symptoms, unremarkable systemic review
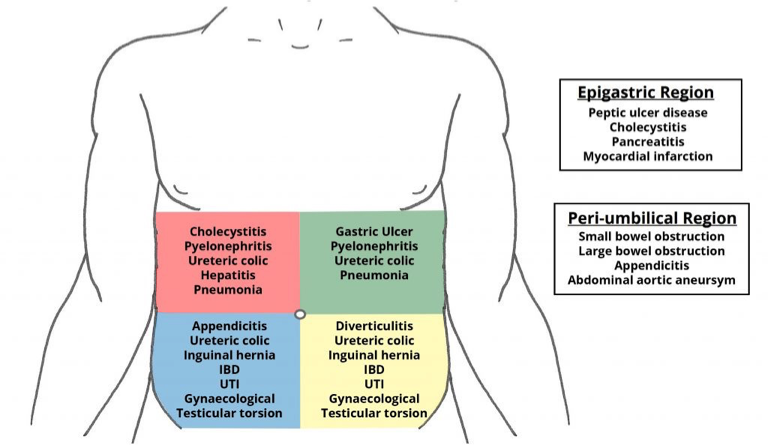
I- Site
Pain wide range - (quadrants)
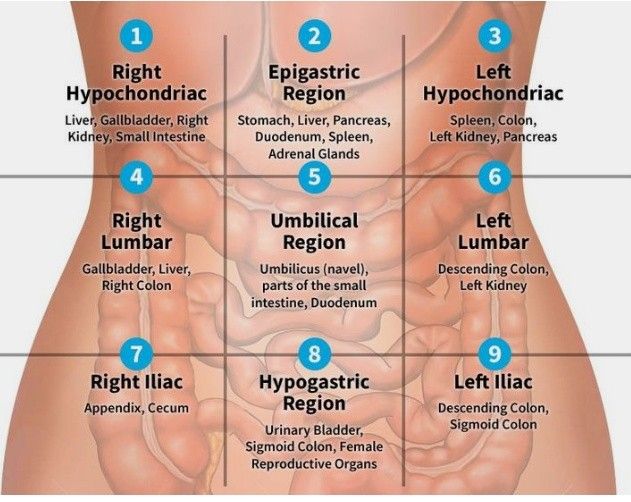
-
Right Hypochondriac
-
Right Lumbar
-
Right Iliac
- Appendicitis, Uriteric colic, pyelonephritis, cecum; IBD)
-
Epigastric
- Peancreatitis, GERD, Peptic Ulcer, Cancer, Deuodenal Ulcer, esophagitis, Left lobe of liver, Myocardial infacrtion)z
-
Umbilical region
-
Hypogastric region
-
Left Lumbar
-
Left iliac
- Divertucilitis
- Sigmoid -
- Ulcer
Important RUQ - rad to shoulder - Chole Epigastric - RAD Back - pancreatitis
| Region | Category | Differential Diagnosis |
|---|---|---|
| RUQ | Hepatobiliary | Biliary colic, Cholecystitis, Cholangitis, CBD obstruction (stone, tumor), Hepatitis, Budd-Chiari, Hepatic abscess/mass, Right subphrenic abscess |
| Gastrointestinal | Pancreatitis, Presentation of gastric, duodenal, or pancreatic pathology, Hepatic flexure pathology (CRC, subcostal incisional hernia) | |
| Genitourinary | Nephrolithiasis, Pyelonephritis, Renal: mass, ischemia, trauma | |
| Cardiopulmonary | RLL pneumonia, Effusion/empyema, CHF (causing hepatic congestion and R pleural effusion), MI, Pericarditis, Pleuritis | |
| Miscellaneous | Herpes zoster, Trauma, Costochondritis | |
| LUQ | Pancreatic | Pancreatitis (acute vs. chronic), Pancreatic pseudocyst, Pancreatic tumors |
| Gastrointestinal | Gastritis, PUD, Splenic flexure pathology (e.g. CRC, ischemia) | |
| Splenic | Splenic infarct/abscess, Splenomegaly, Splenic rupture, Splenic artery aneurysm | |
| Cardiopulmonary | (see RUQ and Epigastric) | |
| Genitourinary | (see RUQ) | |
| RLQ | Gastrointestinal | Appendicitis, Crohn’s disease, Tuberculosis of the ileocecal junction, Cecal tumor, Intussusception, Mesenteric lymphadenitis (Yersinia), Cecal diverticulitis, Cecal volvulus |
| Hernia | Femoral, inguinal obstruction, Amyand’s (and resulting cecal distention) | |
| Gynecological | See ‘suprapubic’ | |
| Genitourinary | See ‘suprapubic’ | |
| Extraperitoneal | Abdominal wall hematoma/abscess, Psoas abscess | |
| LLQ | Gastrointestinal | Diverticulitis, Diverticulosis, Colon/sigmoid/rectal cancer, Fecal impaction, Proctitis (ulcerative colitis, infectious; i.e. gonococcus or Chlamydia), Sigmoid volvulus |
| Hernia | ||
| Gynecological | See ‘suprapubic’ | |
| Genitourinary | See ‘suprapubic’ | |
| Extraperitoneal | Abdominal wall hematoma/abscess, Psoas abscess | |
| Epigastric | Cardiac | Aortic dissection/ruptured, AAA, MI, Pericarditis |
| Gastrointestinal | Gastritis, GERD/esophagitis, PUD, Pancreatitis, Mallory-Weiss tear | |
| Suprapubic | Gastrointestinal | (see RLQ/LLQ): Acute appendicitis, IBD |
| Gynecological | Ectopic pregnancy, PID, Endometriosis, Threatened/incomplete abortion, Hydrosalpinx/salpingitis, Ovarian torsion, Hemorrhagic fibroid, Tubo-ovarian abscess, Gynecological tumors | |
| Genitourinary | Cystitis (infectious, hemorrhagic), Hydroureter/urinary colic, Epididymitis, Testicular torsion, acute urinary retention | |
| Extraperitoneal | Rectus sheath hematoma | |
| Diffuse | Gastrointestinal | Peritonitis, Early appendicitis, perforated appendicitis, Mesenteric ischemia, Gastroenteritis/colitis, Constipation, Bowel obstruction, Pancreatitis, Inflammatory bowel disease, Irritable bowel syndrome, Ogilvie’s syndrome |
| Cardiovascular/Hematological | Aortic dissection/ruptured AAA, Sickle cell crisis | |
| Genitourinary/Gynecological | Perforated ectopic pregnancy, PID, Acute urinary retention | |
| Endocrinological | Carcinoid syndrome, Diabetic ketoacidosis, Addisonian crisis, Hypercalcemia | |
| Others | Lead poisoning, Tertiary syphilis |
II- Onset
Acute
- Peritonitis follower by perforation (dialysis)
- Appendicitis
- Truama
- Rupture Ectopic
- Ruptured Aortic Aneurysm
- Mesenteric Ischemia
- Bleeding ulcer
Chronic Inflammations
- Hepatitis
- IBD
- Chronic cholecystitis
- Biliary colic
Both
- Intestinal Obstruction
III- Character
Colicky, Constant dull aching pain Biliary colic if there’s impaction of stone
**Sharp/Stabbing/
Constrictive
Burning
- GERD
- Peptic Ulcer Disease
Throbbing
- Acute severe inflammation (infections)
- Abcess
Dull / Aching
- Acute cholecystitis (Inflammatory process)
constant Dull aching pain - radiation to shoulder due RT dome diaphragm supplied by phrenic nerve
Colicky Pain (Tubular structures - smooth muscle contractures)
- Stones (gallbladder, kidney, intestinal…)
- Uterine contractions
Biliary Colic type of pain - it comes in goes
- Renal colic
- biliary colic
- urinary colic
Heaviness?
IV- Radiation
- Pancreatitis - RAD to the back
- Spleen - Left shoulder
- Renal colic: to groin
- Cholecystitis - RAD Right shoulder (phrenic nerve)
- Appendicitis - Peri-umbilicus shifting to the right illiac fossa
- Ruptured aortic aneurysm: to back or flank
- Perforated ulcer: to RLQ (right paracolic gutter)
- Hip pain: to groin
V- Associated Symptoms
General abdominal pain Fever, melena, hematemesis colon/biliary cancers - and others depending on differential…
In biliary colic Itching, Fever, maliase , nausea, vomiting, urine, stool
(obstructive jaundice in case pale stool) (Urine dark due liver is normal water soluble goes serum body fluids) (Pre-hepatic insoluble bilirubin - Normal urine & Stool Dark) (steatarohea due ??)
jaundice if someone noticed it do you have itching or dark urine
In Jaundice
- Itching
- dark urine
- dark stools
- weight loss
- fever / malaise
- bruising
VI- Timing/Episodes
General
- More after waking up, waking up in middle of night, more in the afternoon?
- timing, Duration, episodes of free disease.
In biliary colic usually after eating meal
VII- Factors
- relieving factor, sitting position? not eating? after meal?
- Exacberating factors Peptic ulcer GERD - R Milk peritonitis - any movement pain - stand still IBD IBS - Stress factor
In biliary colic Eating especially in Fatty food will increase pain - due bilestone contraction Leading forward? Not eating? Analgesics?
VIII- Severity
1-10 Grading with Limitations - cant walk, work, or think
4) B Symptoms
Fever, Night sweats, Weightloss, loss of apetite
5) Systemic Review
can be after HOPI or past Hx
6) Past Hx
Past medical / Surgical / Family
-
similar episode as before similar problem - (you can mention with HPI)
-
Chronic diseases + Family Hx / similar conditions Pancreatitis, bleeding peptic ulcer or inflammatory bowel disease, stones.
-
Past Admission + transfusion + Surgeries Important to ask about previous abdominal surgery and if there were any complications during or after surgery
-
Pregnancy / Lactation
Medications / Allergies
-
Medication (name/dose/side effects)
- Antibiotics cause diarrhea
-
Allergy
Social im going to ask some specific question to reach to diagnosis, may i?
- Occupation,
- Travel,
- kids,
- smoking,
- alcohol,
- drugs,
- sexual activity
Other Hx presentations of past Hx
In biliary colic
Past Medical: recurrence, DM, HTN
Past Surgical; cholecystectomy, previous stone removal
Drug abuse: Alcohol, Travel (malaria),
…
In Jaundice CLD, Hematological, IBD, GB diseases Paracetamol, steroids, Anti TB Social: alcohol / smoking
7) Summary
77 yo sudanese male complaining of abdominal pain for 9 days which was severe compressing radiating to back associated with cough, with no hx of palpitation, syncopal attack - with hx of cabg.
8) Differential, Impression, most likely diagnosis
- Pancreatitis
- Gastric Ulcer
- biliary colic
- …
Then justify - most likely diagnosis follow through with directive investigations
9) Investigations
The investigations in all cases of the acute abdomen share the same generic outline:
Labs
- Routine bloods – FBC, U&Es, LFT, CRP, amylase
- Calcium in suspected Pancreatitis.
- Blood cultures – infection
- Lactate, Troponin
- Urine dipstick – infection/hematuria ± MC&S.
- Urine Analysis
- B-HCG pregnancy test - for all women of reproductive age.
- ABG – useful in bleeding or septic patients, especially for the pH, pO2, pCO2, and lactate for signs of tissue hypo perfusion, as well as a rapid hemoglobin.
- Note: Any amylase / lipase 3x greater than the upper limit is diagnostic of Pancreatitis. if lower than 3x it may indicate perforated bowel, ectopic pregnancy, or diabetic ketoacidosis (DKA)
Imaging
ECG In the emergency setting, every patient with abdominal pain should have an ECG to exclude myocardial infarction. Other imaging modalities that may be initially requested include:
Ultrasound:
- Kidneys, ureters and bladder (‘KUB’) – for suspected renal tract pathology
- Biliary tree and liver – for suspected gallstone disease
- Ovaries, fallopian tubes and uterus – for suspected tubo-ovarian pathology
Radiological:
- An erect chest X-ray (eCXR) – for evidence of bowel perforation.
- CT imaging, depending on the suspected underlying diagnosis
KEY TESTS FOR OR SURGICAL PREPARATION
- CBC, electrolytes, creatinine, glucose
- INR/PTT
- CXR (if history of cardiac or pulmonary disease) bowel perforation
- ECG if clinically indicated by history or if >69 years and no risk factors - MI
in biliary colic
Blood tests: (complete blood count, liver function tests and serum amylase) will be normal
Imaging: Ultrasound abdomen will show the gallstones with acoustic shadowing.
in Jaundice
-
CBC (leukocytosis; obstruction, RBCs)
-
LFT (ALT AST ALP GGT Amylase…)
-
Coagulation profile (increased prothrombin in obstruction - deficient liver vit K)
-
Lipid Profile
-
Viral profile (hepatitis/Hiv)
-
U/S - size CBD (gallstone, carcinoma), acoustic shadow, thickness wall, distended, collapse, tumor in pancreas
-
ERCP - endoscopy, deuodenum, ampulla vater, dye is injected - to see any strictures or stone - stone can be retrieved - retrograde
-
MRCP - Diagnostic - intra/extra hepatic biliary tract imaging
-
CT - cancer, staging, malignancy
-
PTC - TANSEEM; used in severe cases of bilirubin to decompression - ?? -
10) Treatment Plan
General Acute Abdomen Depends on diagnosis and findings
in biliary colic cholecystectomy
In Jaundice Depends on the cause
- Choledicocholethiasis - ERCP if fails open surgery
- Carcinomas - chemotherapy, surgery depending on stage/operable diseases
- Head Pancreas carcinoma - Whipple’s surgery
Q&A Jaundice
Prehepatic: hemolysis, Malaria
- normal hepatic function - high indirect bilirubin
- urine & stool normal
Hepatic: Liver cirrhosis, Viral Hepatitis,
- Fever + malaise, Organomegaly
- ALT & AST ratio is higher
- Total bilirubin raised
- ALP is normal?
Post-Hepatic: Obstruction (Stones, head pancreas, carcinomas, strictures, inflammatory conditions; cholangitis, ((((((perampilliary tumour around the ampulla of vater - oppening both cbd????) ))) ((2cm pearmapillary tumour - maybe cancerinoma of ampulla of pancreas or bile duct or deuodenmum??)))))
Internal Obstruction… External obstruction - carcinoma head pancreas, LN’s in portal triad
- Jaundice, pleuritis, (Itching??)
- ALP, GGT high
types of stone and its location list?
stool & urine color depending on hepatics
Other Notes
gallbladder palpable - carcinoma ? Corviesar law? - distendended gallbladder suggested carcinoma
not palpable - in stone due to reccurent stones resulting in fibrosis
Charcot Triad (jaundice, Tenderness, RUQ, Fever)
Pentad (Triad + confusion + Hypotention)
typical presentation head pancreas - painless progressive jaundice
CCTD EXAM
Framework
-
WIPER
- Wash hands
- Introduce
- Right side of bed
- Explain Procedure
- Permission for examination
- Position & Exposure
-
Preliminary examination
- General Appearance (man, comfortable, comatose, connected device)
- General examination (Vitals, hand/arm/axilla, hair, face, neck, chest, abd,leg)
-
Focused Examination + (correct technique)
- Specific System Exam - IPPA
- Inspection
- Palpation
- Percussion
- Auscultation
- Lesion/Swelling/Ulcer if present - SSSS TTEDC
- Specific System Exam - IPPA
-
Describe correct physical findings
Totally 6 minutes for full examination
1) WIPER
Exposure | position | privacy | Ask for vitals
- W ash hands (before and after)
- I ntroduce yourself to the patient and seek his or her consent
- P osition the patient correctly.
- E xpose the patient as needed (e.g. ‘Please take off your shirt for me now, if that is all right’)
- R ight side of the bed
Position & Exposure Abdominal (liver) exam: Supine - Mid nipple to mid thigh - cover genitalia
Neck exam: Sitting - Chin to Nipple line
Peripheral Vascular Disease exam: Normal intro than exposure (bilateral lower limb and cover genitalia position is sitting or semi sitting)
Breast exam:
Semi-recumbent position - upper umbilical and above
Intro
Greet, Introduce (5th year med), assure privacy (curtain, nurse), explain procedure, position (mention good position - supine semisitting) & exposure (from midchest to midthigh - cover genatelia)
In the end thank the patient document.
2) General Appearance
- Conscious and alert
- features
- connected devices
elderly male with good build lying comfortable to be - connected to cannula - not connected oxygen. (note general exam findings)
adult sudanese male lethargic, in bed not connected to any device.
conscious alert man, well built, healthy, looks comfetable laying on bed, connected to vitals signs, no iv canulla, no oxygen, no foleys
In neck exam Agitation, nervousness or lethargy, myxedema,
“Now i will do focused examination after general apperance, should i do general examination?”
Is the patient well or unwell, comfortable or in pain, moving easily or lying motionless? e.g. peritonitis?
Writhing in agony, e.g. ureteric or biliary colic?
3) General Examination
dont touch patient until needed
-
Vitals
- Temperature
- Pulse: Tachycardia, bradycardia, water hammer pulse
- BP & RR
-
Hand: organized explaination from distal to proximal
- distal - nail, feature…
- no janeway.. no osler node…
- specific - cardiac, GIT, Resp
- no infection, no swelling, no deformitiy in dorsum
- no palmar erythema: liver cirrhosis, mitral stenosis , rheumatoid arthritis
- No janeway lesion: CVS
- Leukonechia kolionechia
- Clubbing (window test); Hypoxia; angiogenesis many causes— likely resp cvs, congenital heart diseases, malignancy
- Rheumatoid deformity w/ ulnar deviation - Z shape thumb, fixed not correctable - ((swan neck vs boutonniere??)), guttering.
- Sweaty; Hyper
- Thick: Depature contracutre???, hypothyroidism
- Dry: hypo
-
Clubbing - window test
-
Capillary refill
-
Pulse: (rate | rhythm | character | volume | comparison | radioradial delay)
- Dorsalis pedis
- Medial Malleolus
- Popliteal arteria
-
water hammer pulse
-
Vital signs - BP, RR, Temp, Pulse, saturation, - mention need to check
-
Face & Neck: head to neck
- general appearance
- Hair: normal hair distribution
- eye: no pallor/jaundice
- Nasal: no nasal discharge
- Mouth: oral hygiene, central cynosis, oral ulcers
- Neck: no obvious thyroid LN JVP, cyst, swallow - want me to examine?
-
Abdomen: general palpation -
-
Lower Limb: Edema - thumb
Edema Grading- GRADE I: edema from dorsum of foot & then behind medial malleolus bilateral;
- GRADE II: Tibial
- GRADE III: Pinching, catching fold of skin on thigh to check edema
- GRADE IV: Antero-Abdominal wall; peduea orange appearance, thick, red +++ Sacral edema; ascites ((generalized anasarca?))
Abdominal (liver): Water hammer, jaundice, Spider novae, gynecomastia
axilla acanthosis nigricans indicating GI Malignancy, Abdomen, Edema
Neck: Whole Patient Agitation, nervousness or lethargy, myxedema,
Hands sweating, tremor, tachycardia, dry, irregular pulse/temprature, palmar erythema thyrotoxicosis - fine fast tremor
Eyes lid retraction, exophalamos, lid lag H test, ophthalmoplegia, chemosis Ophthalmoplegia, particularly of the superior rectus and inferior oblique muscles (cannot look ‘up and out’) Exophthalmos, which also causes difficulty with convergence and absent forehead wrinkling when looking upwards
Neck
- Lump moves with swallowing? protrusion of tongue?
- skin
- scar transverse cervical incision
Palpate Cervical LN’s
Extremities
- edema
Peripheral Vascular Disease: Start with general examination (Inspection and vital along with patients looks) Describe the dressing site and looks (ask the doctor to remove the dressing)
no pallor (check eyes for pallor - look up), hand no tar staining
Breast:
- Chest: any effusion
- Abdomen: hepatomegaly, ascites
- Spine: pain, tenderness, limitation of movement
4) Focused Examination
Lesions/Mass/Ulcer Examination
I- Comment on lesion if found while examining anywhere in body, ask instructor to Start its own inspection palpation auscultate percussion then continue with previous focused examination
- Site (right neck swelling, lateral of second toe)
- Size (0.2x0.8 Meters/cm use ruler)
- Shape (Irregular, regular (round), Oval)
- Surface/Base (feel surface Nodular or Smooth)
- Depth (Deep or superficial - check contraction after squeeze hand)
- Color/Floor (strawberry, portwine?, purple, orange, chronic inflammation; hyperpigmentaiton, redness; active inflammation) (thick granulation tissue with slight oozing of serious discharge) i. Red/Pink: This indicates granulation tissue. Granulation tissue indicates healing. ii. Slough (Yellow Like Cotton): Dead tissue separating; it’s almost going to die. iii. Black: Indicates necrotic tissue. If applicable, we can also say ‘expose tendons or exposed bone’
- Temperature ( Hot; Abscess, Malignancy , Cold, Normal; Lipoma)
- Tenderness (Painful or Painless)
- Edge (Ill-defined or well-defined or Sloped) (Punched out or Under Minded?) ALL EDGES IN DIABETIC FOOT ARE SLOPPING EDGE/HEALING
Lesion/Mass SSSS C TTED Ulcer SSS BEF + Surrounding Floor by inspection in ulcers feel base by palpation in ulcers
II- Composition: Solid, fluid or gas
- consistency (Hard/Firm/Soft like?) (soft if pheripheral??)
- fluctuation (Fluid; Cyst - Pseudocyst; without epithelium Push two fingers against another in between pressing from above) (Cystic push in central)
- fluid thrill ()
- translucence (Torch; hydrocele - any cyst vs hernia)
- resonance
III- Mass Pull skin to see if its attached to skin (such as sebaceous cyst) (video?)
put your fingers in between sternocleidomastoid to separate mass (video?) - attached to muscle
IV- Vascular
-
pulsatility (Transmitted/True? - aneurysm, varicose) - Expansile vs transmission (two finger))
-
compressibility (Tumour/Hernia/)
-
bruit (Turbulence/Murmur - thrill if palpable)
- Reducibility (Renal Hernia, cough)
- Relations to surrounding structures – mobility/fixity
- Regional lymph glands (Malignancy/Infection — Primary / Secondary
V- State of local/Surrounding tissues:
- scars/edema
- Arteries (examine arteries before & after the swelling (Parathesia, loss of pulse etc..))
-
nerves - cotton, pin prick, position/vibration sense etc…
-
Bones and joints
Abdomen Focused Examination
Abdominal Inspection
Go in-front patient check for
-
hernias (Cough)
-
Umbilicus (everted or inverted?)
-
Symmetrical
-
Hair distribution
-
pigmentation
-
Visible masses
-
Scars / Surgical / tattoos
- Renal transplant Scar - located at Appendix right iliac fossa
- Kocher scar
- Midline scar
-
Deformities
-
Distention; 5 S’s (normally mild convex)
-
Fluid; Ascites
-
Fat
-
Flatus; Gas
-
Fetus
-
Fibroid - Mass
-
-
Abdominal movement with respiration
- Male - Abdomino thoracic
- Female - intercostals stronger
- Obstruction (intestinal / Gastric) perlstatic movement
- Pulsation (tumour / )
- Hernia (Cough - Bulging appear)
- Positive expansile impulse
- Umbilicus (Position “Central, shifted; due tumor”, evert, invert, discharges; pus, urine, fistula, etc…, skin; hair distribution, scars, cushing, cullen’s sign, caput medusa “central Portal HTN” peripheral IVC obstruction)
-
Lower limbs: Edema, hernias…
Pitting Edema (CLD) - warm your hand before palpation - press with two sides at same time for bony prom of tibia, check patient eyes for any pain - comment findings
Visible Mass comment on LESION
Abdominal Palpation
Essure good technique (full hand relaxed on patient + good percussion)
Superficial Palpation Do you have any pain in abdomen - start far away from site of pain - look at the patient eyes to check any tenderness
Palpate 9 quadrants anti clock wise starting from left iliac or far away from pain site
- Tenderness
- Gaurding
- Palpable mass
Deep Palpation - after inspiration palpate the areas
- Organomegaly
-
Hepatomegaly - Edge + Tenderness + liverspan (percussion) (confirm with chest percussion, then reconfirm percussion on abdomen for dullness after palpation) - Edge (sharp round?) surface (nodular, smooth?) Liver span is normally 6 to 12 cm in the midclavicular line
-
Pyelomegaly - bimanual - (costo-vertebral angle)
-
Splenomegaly - Oblique growth (Renocolic; splenic flexture) (use tips of hand on direction oblique more to palpate the spleenomegaly from LRQ obliquely to spleen site) - not palpable in healthy, palpate in wave form from tip of finger after deep breath
-
Cholecystitis - Murphy’s sign (Catch breathing)
-
How to differentiate kidney, spleen
-
Spleen has notch, enlarges Diagonally/Oblique, moves with respiration, not palpable, under rib cage cant go above it
-
Kidney enlarges Vertically, largely unrelated, Palpable , Ballottable, does not move with respiration
Abdominal Percussion
-
Organomegaly (differentiating organs and extent),
- Spleen & Liver Dull
- Kidney is resonant; bimanual
Liver size Start below then above costal margin by cm or finger width
-
Fluid thrill & Shifting dullness Shifting Dullness Percussion from below sternum - until dullness from bladder - then becomes resonance, change position of hand to vertical by then https://www.youtube.com/watch?v=Eog7addNRwc M ild to moderate ascites are usually on flanks - You can check by percussion -
-
dullness progressively getting more by flanks Light percussion middle midline for shifting dullness - Between 3rd and 1st space between umbilicus then percussion rest check for ressonance/Dullness
-
to assure its ascites or mass; keep hand same position by 20-30 seconds;
-
do the percussion again after shift other side, then after 10 seconds for viscera of fluids to descend - percuss to check… switching patient to other side; if mass it will be dull - if ascites the fluid directed downwards resulting in shifting dullness & resonance - reverse shifting dullness? Ascites? if huge Fluid Thrill
Fluid Thrill bilateral test flick, not advised Severe ascites, will resulted in … 1. main indicator by simple touch, with slight movement of abdominal region 2. Put hand on other side, and stimulate the abdomen from opposite side - (((whilst asking patient put their hand in midline))); to prevent transmission of fluid through anterior abdominal wall
Resonance tympanic,
AUsc Perstaltic movement, aneryusm,
Costophrenic percussion
Abdominal Auscultation
Peristaltic movement, aneurysm, bruit
-
Bowel sounds: Healthy persons may have no bowel sounds for several minutes (silent intestinal contractions). Bowel sounds are exaggerated (borborygmus), and increased in rate in mechanical intestinal. Absent (paralytic ileus),
-
venous hum: (indicate portal hypertension) - soft systolic murmur - large volume of blood flows in umbilical and paraumbilical veins in falciparum ligament (portosystemic shunt)
-
hepatic bruit: (indicating increase vasculature) - Heard over the liver, usually due to hepatocellular carcinoma, or vascular hepatic tumours
-
Aortic bruit: Just above the umbilicus
-
Renal bruit: Occurs in renal artery stenosis due to turbulent flow through a narrowed vessel
-
Succussion splash: Excess fluid in the gut, e.g. from pyloric stenosis, or advanced intestinal obstruction, may splash when the abdomen is shaken, or the patient rolled from side to side
Neck Focused Examination
Neck Inspection
-
at same level - check for wounds, sinuses, discharges, neck vein distension (Pemberton’s sign; raise both arms), discoloration; hyperpigmentations
-
check from sides (to check visible pulsations, bulging)
-
Movement from swallowing (This indicates it is deep to the pretracheal fascia and likely to be thyroid. (thyroid, lymph nodes pretracheal fascia)
-
Protrusion of tongue (thyroglossal cysts)
Neck Palpation
Infront Patient
-
Tracheal deviation/position - 2 fingers placed on head clavicle w/ middle finger on rings of trachea.
- once hands are placed you would feel tracheal position then comment.
Behind
-
palpate three fingers against one side of lobe pushing the other against it - ask patient to swallow (give water). dont move both hands at same time. then palpate while patient protruding his tongue
-
Palpate lower pole/edge of thyroid/mass to exclude retrosternal goiter - if its positive non palpable its retrosternal goiter) -
-
Comment on lesion (solitary in one sided? toxic solitary?)) - comment on lesion as previously mentioned S4 DECTT,
-
Comment on palpation lesion/Thyroid - follow through with Lesion format in inspection
- Site
- Size
- Shape
- Tenderness -by staring at patient eyes from behind at all times
- Temperature - of each side - compare with sternum
- Number
- Consistency (Fluctuation; Cystic or firm)
- Surface
-
Thrill by palpation - bruit by asucultation
-
pulsation is seen - is it transmitted or expansile?
-
Carotid/ superficial temporal Pulsation - carotid pulse is present but deviates - if both not felt = malignant (berry’s sign)
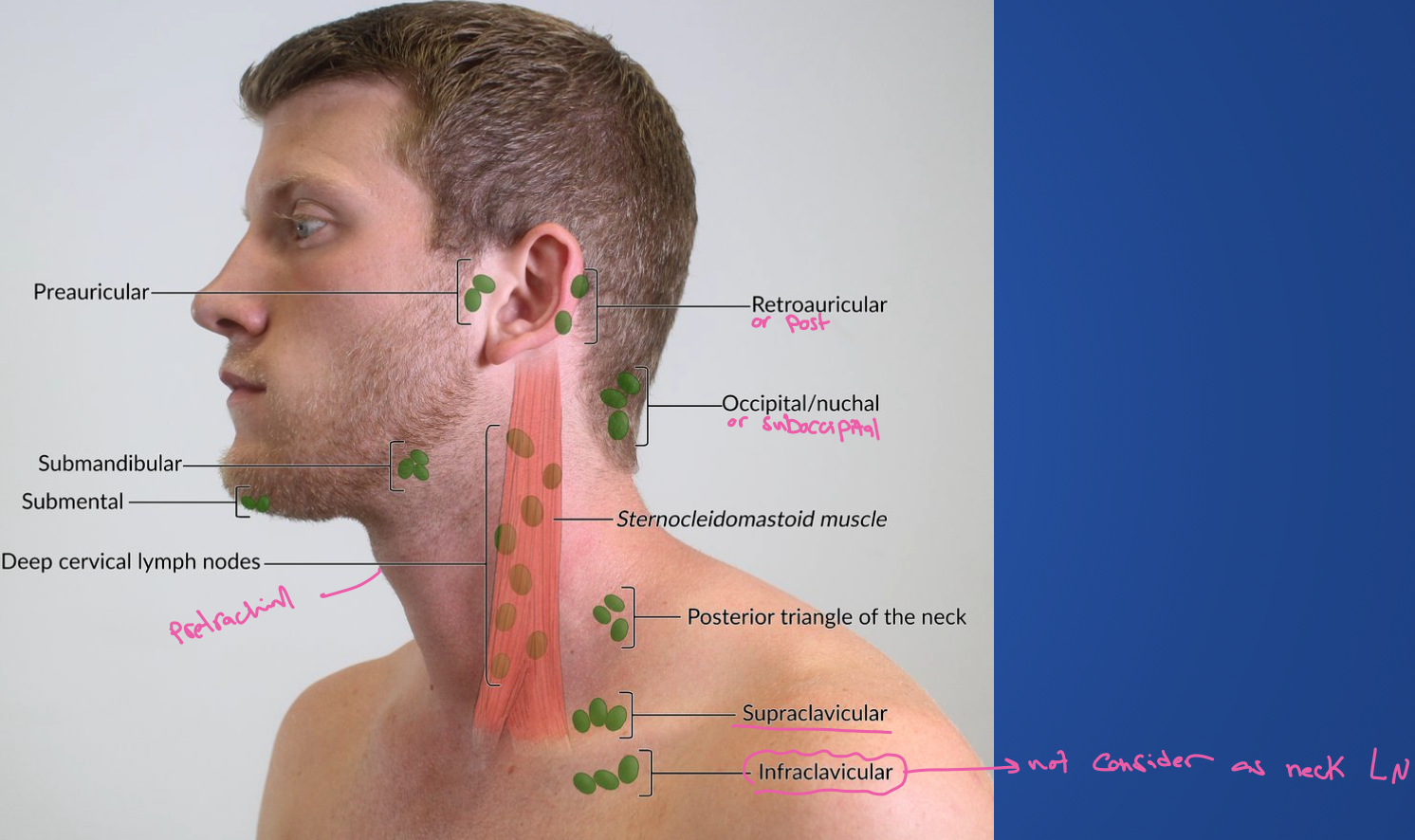
Lastly behind patient examine LN’s Neck (submental, submandiublar, pre-pot auricular, sub-occipital, Anterior/Deep cervical, Post/Superficial cervical supraclavicular)
Clinically, Lymph Nodes are arranged in 2 Main groups: Transverse - Submental, Submandibular, Pre and Post Auricular, and Occipital.
Longitudinal – Cervical group (Anterior and Posterior Cervical), and Supra-Clavicular Listening for Bruiting is required for the Neck examination, but not for the Thyroid. As the Carotid Artery is part of the neck.
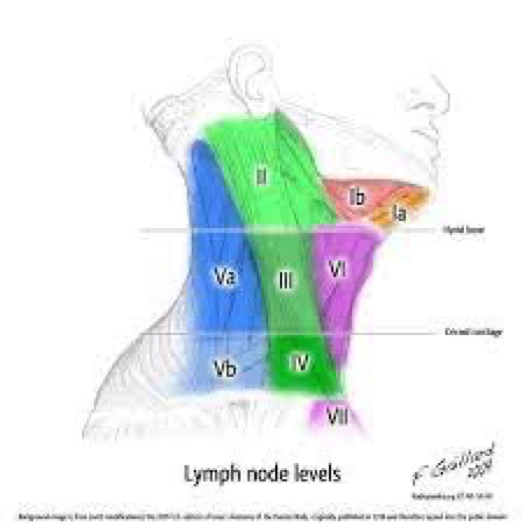
-
I- submental submandibular
-
II, III, IV - Sternoclediomastoid
-
V- Post Sterno
-
VI - Pre Sterno
-
VII - Sternum
Neck Percussion
three fingers on manubrium sterni Percuss from sternum with one hand - any dullness - retrosternal goiter
Neck Auscultation
- Auscultate both lobes to check for any Bruit.
- carotid auscultation
Peripheral vascular Focused Examination
Peripheral vascular Inspection
- Inspect infront bed patient,
- to inspect, check between foot fingers,
- raise legs to see any hidden ulcer
General findings of Peripheral vascular disease (typically pale hair loss atrophy erythema skin break down wound nail changes )
theres gauze medial on surface of foot, the gauze is soaked with (pus yellow, clear fluid) dressing is clean? (clean) - ask examiner if you can remove the gauze..
Comment on
-
there is hair loss and
-
no ulcer look between toes and under the heal
-
(usually ulcer is punched out in DM look for edge and floor most importantly than others also site and etc) (move everywhere)
-
Amputations, lumps, scars, scratch marks, muscle atrophy, symmetry
Comment on Ulcer if found
-
Site (lateral of second toe)
-
Size (2x2 cm)
-
Shape (oval/rounded/irregular)
-
Floor by inspection floor you can see, base you can touch. We must describe the colour of the floor:
i. Red/Pink: This indicates granulation tissue. Granulation tissue indicates healing.
ii. Slough (Yellow Like Cotton): Dead tissue separating; it’s almost going to die.
iii. Black: Indicates necrotic tissue. If applicable, we can also say ‘expose tendons or exposed bone’.
-
Base (surface) by palpation
-
Edge (Punched out or Under Minded?) ALL EDGES IN DIABETIC FOOT ARE SLOPPING EDGE/HEALING
-
Surrounding (edematous, discharges, hair distribution…)
SSSS BEFS
Then look for any discharge by squeezing above and below ulcer looking for discharge also look for base and edge again also fluctuation test looking for tenderness and temprature
Peripheral Vascular Disease Palpation
I- check tenderness & temperature on all levels of lower limb from foot tibia thigh right and left (compare both limbs with dorsum of hands) (press on each level look patient eyes, ask patient if he noted any pain)
II- Pulse examination (examine one side each)
- dorsalis pedis (assessed by tarsal bone lateral to hallicus longus)
- Posterior tibial (medial malleous two cm posterior midway below)
- Popliteal & Femoral Pulse
III- Capillary Refill
- compress finger (hold finger then compress nail bed - 2-3 seconds)
IV- Edema assess levels from tarsal prominence, medial mal, tibia, thigh, sacrum
V- Beurgers test
-
Patient Position: Supine (lying flat on their back).
-
Pain Assessment: Ensure the patient is not experiencing any lower limb pain at rest before starting the test.
-
Leg Elevation:
- Passively elevate the patient’s left leg to 10 degrees.
- Hold for 10 seconds and observe the color of the foot, particularly the plantar surface (sole).
- Incrementally elevate the leg by 10 degrees every 10 seconds until reaching a 45-degree angle - normally at 90 degree there is pallor - ischemia at 20 degrees pallor will appear
- Throughout elevation, watch for pallor (paleness) developing in the foot.
-
Dependency:
- Once the leg is at 45 degrees, ask the patient to sit up and dangle their legs over the edge of the examination table.
- Observe the color of the foot as it becomes dependent (hanging down).
- Look for reactive hyperemia (redness) as blood flow returns to the foot.
-
Interpretation:
-
Positive Buerger’s Test:
- Marked pallor develops during elevation.
- Delayed or absent reactive hyperemia (redness) upon dependency.
- These findings indicate significant arterial insufficiency.
-
Negative Buerger’s Test:
- Minimal or no pallor develops during elevation.
- Rapid reactive hyperemia (redness) upon dependency.
- These findings suggest adequate arterial flow.
-
-
Repeat: Perform the same procedure on the right leg.
Peripheral Vascular Disease Percussion
No percussion
Peripheral Vascular Disease Auscultation
Auscultation Sites for Peripheral Vascular Disease:
-
Femoral Artery:
-
Location: Auscultate at the mid-inguinal point, which is halfway between the anterior superior iliac spine (ASIS) and the pubic symphysis.
-
Significance: This is the most accessible point to assess the femoral artery for bruits, which are turbulent blood flow sounds indicative of potential stenosis or occlusion.
-
-
Iliac Artery:
- Location: Auscultate in the iliac fossa, a region located deep within the lower abdomen. This requires deeper palpation and may be challenging.
- Significance: Bruits heard here can suggest stenosis in the iliac artery, potentially impacting blood flow to the entire lower limb.
-
Hunter’s Canal (Adductor Canal):
-
Location: Auscultate along the medial surface of the thigh, midway between the groin and the knee. This is where the femoral artery travels deep within the Hunter’s canal.
-
Significance: While not routinely auscultated, bruits here can indicate stenosis within the femoral artery as it passes through this confined space.
-
Peripheral Vascular Disease Complete examination with
Inspect then Motor (power and tone) , Sensory(position and vibration sense, pinprick, cotton test), Reflexes (babinski, achilees, patellar)
Breast focused Examination
Breast Inspection
Inspect three levels while on
- At Rest
- Raised Arm,
- Arm to waist, and
- below folds
Comment on
-
assymetry - level - visible mass? - s?
-
Skin changes? Colour? texture of nipples (peduea orange; thick edematous skin - due lymphatic drainage blockage)
-
Nipple areola complex nipple retraction due mass behind niple - (could be physiological)
- Carcinoma (retraction)
- Paget’s disease (ulceration) raised level, retraction, ulceration
-
Discharge,
- Red: Ductal papilloma, carcinoma
- Yellow/Green: Fibrocystic disease, duct ectasia
- White/Milky: Galactorrhea
- Pus: Abscess
-
affected areas (unilateral, bilateral? which quadrant?)
-
vissible masses
-
Dilated veins
-
PAC RING
-
ulcers
-
cooper ligament holding structure of breast - skin dimpling - due fibrosis of malignant cells infliltration to cooper ligament
Lymph node inspections Its important to mention Mobility, Attachment
-
raise arm and to waist Examine the axilla
-
Then Inspect the supra/infra clavicular area - involved in level 3 (medial) stage
-
infammary lines, protraction of pectrolaris muscle to see any dimpling
Breast Palpation
I- Palpation of Breast
- raise arm
- to waist
- below folds
- Palpate axillary tail (contains breast tissue) infront pectoralis major edge axilla
Palpate the 4 quadrants for any obvious mass or lump. first on normal side fully then compare. palpate with palmar
clockwise palpation to check any masses/tenderness solid hard mass, irregular margin, immobile.
Comment on swelling/lump same as Lesion identification
-
Lump characteristics: site, size, shape, surface, mobility, temperature, tenderness, texture, edge, attachment to skin or deep tissue For these characteristics - use the pulp of your fingers\
-
Site: More carcinoma develops in the upper outer quadrant
-
Size: Variable, Large mass - giant fibroadenoma, Phylloides tumor
-
Shape: Well defined - fibroadenoma, ill-defined - carcinoma
-
Mobility: Fibroadenoma freely mobile
-
Temperature: Raised in inflammation, inflammatory carcinoma
-
Tenderness: Inflammatory – abscess
-
Texture: Hard - carcinoma, firm - fibroadenoma, fluctuant - cyst
-
Attachment: Carcinoma, sometimes inflammatory lesions
Comment on Skin tethering - tumor infiltration of Cooper’s ligament pulling on the skin. Skin dimples when the tumor is moved to one side or arm raised above the head.
Skin fixation - when the tumor is directly fixed to the skin. The skin cannot be moved/pinched separately.
Muscle attachment - patient’s both hands resting on hips, test lump mobility before & after muscle contraction (ask the patient to press against hips).
superior inferiot movement of pectrolaist major if theres mass fixed to muscle
II- Palpation of aeoral complex
- Any retraction/ulceration
- Palpate for a mass underneath the affected nipple
- Nipple discharge - blood (red), serum (brown, green, straw-coloured), pus, milky
- Pathological discharge: Bloody, spontaneous, unilateral
- Discharge spontaneous or on pressure of a segment of the areola
- Any mass associated with the discharging duct
III- Palpation of lymph nodes
Shake hands hold it with patient with your dominant hand, palpate with your left resting on forearm to relax pectoralis major for palpation
-
Axilla, supraclavicular, infraclavicular lymph nodes
-
Patient sitting upright
-
Rt. Axilla: Hold the patient’s right elbow in your right hand. Palpate the axilla with your left hand. For the apex of the axilla, press the finger pulp upward and medially.
-
Lt. axilla - reverse
-
Palpate for supraclavicular, infraclavicular lymph nodes
-
Size, number, and fixation of lymph nodes
-
Examine the arm for any swelling
if contracted lymph nodes will go inside
Axilla contents
- branches brachial plexus
- axillary vessels
- fibro fatty tisues, to give shape
Examine the following anterior group lymphndode behind pectrolist press gently circular movement to feel it promiment
posterior group infront lattismus dorsi
medial on ribs
lateral on head of humerous
apical against center of axilla
infra supra clavical palpate
5) Complete examination with
Mention
Abdominal Exam
- Lymph nodes,
- lower limbs,
- Per Rectal examination,
- Per vaginal if female
- Melenas,
- Temperature,
- Sacral Edema
Neck Exam
- CVS- sinus tachycardia/ fibrillation
- Respiratory system: Tumor, TB
- Abdomen: Hepatomegaly, splenomegaly, other mass, testis
- Extremity- proximal muscle weakness, pretibial myxedema (thyroid dermopathy) – localized lesions of the skin from the deposition of hyaluronic acid
Peripheral Vascular Disease exam
i will finish examination with neurological exam & upper limb peripheral
Breast Exam
- Chest: any Lung effusion
- Abdomen: hepatomegaly, ascites
- Spine: pain, tenderness, limitation of movement
- B symptoms
6) Summarize Findings
…
7) Differential, Impression, most likely diagnosis
Based on findings
8) Investigations
Surgical
- CBC
- Coagulation profile (INR, Prothrombin)
- LFT (metastases) & KFT (contrast)
- Electrolyte (calcium; malignant hypercalcemia)
- Albumin
Abdominal Investigations
…
Neck Investigations
Depending on findings
- Ultrasound
- Radionuclide scan
- Fine Needle Aspiration (FNA) — shows malignancy
Peripheral Vascular Disease Investigations
- CBC
- Sample
- Urine
Breast Investigations
- mammography (more fatty - old age 40 and above)
- U/S (more dense - young) differentiate cyst, mass, suspicious LN
- Chest X-ray.
- Bone scan (spine).
- CT scan.
- Ultrasound (liver).
- CT abdomen.
- If early stage: Bone profile, LFTs.
grade of mammorgam birad 1-6 scores classifcation - indications for biopsy depending on features of the mass
5-6 likely only for biopsy (in this case) Do fine needle aspiration / core needle biopsy
- Core bipsy?, receptors, ER, Progestrin, HER
- FNAC - breast cancer cell not diagnostic
invasive ductul carcinoma grade 2
- CT abd chest, all
- Nuclear PET Scan
Sentinel Lymph Node Biopsy:
- Sentinel lymph node collects lymph from all breast lymph nodes and enters the axilla.
- Blue dye or radioactive isotopes are injected to identify the sentinel node.
- Allows for targeted lymph node removal and reduces the risk of lymphedema.
Adrenal Gland:
- May produce estrogen from androgens.
Staging
- TNM Classification:
- T (Tumor Size):
- T1: < 2cm
- T2: 2-5cm
- T3: > 5cm
- T4: Any size with invasion (edema, ulcer, skin changes, peau d’orange).
- N (Lymph Node Involvement):
- N0: Non-palpable.
- N1: Any palpable, mobile lymph node.
- N2: Fixed lymph node.
- N3: Supra/infraclavicular spread.
- M (Distant Metastasis):
- M0: No distant metastasis.
- M1: Distant metastasis to any structure.
- T (Tumor Size):
Biopsy
-
FNA: (Differential not specified).
-
Core biopsy: Can differentiate invasion of submucosa and mucosa (in situ). Malignant if spread to vessels.
-
Sentinel Lymph node during surgery - vessels will be visible - it will hold the coloring filters it, where it would be location of the sentinel - inject isiotiopes use pencil to check - will give sound
9) Treatment/Management Plan
Depending on findings
Ulcer
VAC (vaccum assisted promote healing) debridement if necrosis
Breast treatment/Management
calcification, structure, surgical plan for calcification mastectomy in this case due prophylaxis to positive genetic makeup
lobectomy if only lump mass found at place.
Treatment Plan:
- Multidisciplinary team approach.
Systemic Therapy:
- Chemotherapy: If breast receptors are not responsive to estrogen.
- Targeted Therapy: Immune therapy (e.g., Her2 targeted therapy) with antibodies and chemotherapy.
- Hormonal Therapy: Tamoxifen.
Surgical Management:
- Breast: Lumpectomy, mastectomy (with or without breast preservation).
- Axilla: Axillary lymph node dissection.
Historical Approach:
- Radical mastectomy (no longer standard practice).
Surgical Cleaning:
- Performed on the patient.
Axillary Lymph Node Removal:
- May result in edema.
before surgery - neo adjuvant therapy post surgery treatment - adjuvant therapy
-
axilla is negative in all imaging - take sentinel lymph node biopsy (first group of LN, pick with gamma probe, then study when frozen - check if theres metases for indicatiative axilla dissection) - sentinel is used when no evidence but cancer
-
2 & 3 suspectious LN - METS - Axillary dissection
Other notes
Neck swelling
Multiple lumps are invariably lymph nodes
A single lump: In the anterior triangle that does not move with swallowing
Solid:
- A lymph node
- Carotid body tumour
Cystic:
- Cold abscess
- Branchial cyst
In the posterior triangle that does not move with swallowing Solid:
- A lymph node
Cystic:
- Cystic hygroma
- Pharyngeal pouch
Pulsatile:
- Subclavian aneurysm
In the anterior triangle that moves with swallowing Solid:
- Thyroid gland
- Thyroid isthmus lymph node
Cystic:
- Thyroglossal cyst
Peripheral
if you dont feel pulse (weakflow)
- check next level
- use hand held doppler (will assess flow in vessel - gives sound)
chronic - diffucult hx due no pain
Breast
Tenderness is found in breast pain such as
- Fibroadenosis
- Premenstrual pain
- Access
Staging T tumor site N lymph nodes involved M metastisis
staging for diff?
-
5x5 mass hard immobile irregular mass with nipple retraction, axilla/supraclavical negative
-
early stage breast cancer
-
surgical duct excision
risk factors to know
- 3 years of contraceptive use
- early menopause (ask age of menarche)
- Nullaparity
- famiily hx of genitoutinary cancers - BRCA - HER2
- previous cancer
CCTD SKILL
Note the patient is amm ahmad, always act! dont say i will do…
CCTD 1 SK Scrubbing & Suturing
Scrubbing
-
Remove all foreign body’s - scratch previously
-
Hand - palm palm, palm dorsum, between fingers, interlock, thumb, tips, forearm (up to down from proximal to distal until elbow) - three times (last forearm till wrist?) - raise arm DUA/MONK
-
Gown -
- given by nurse - give hug to sleeves - find two behind danglers and connect
- If no nurse is present - let it go, hold from tip, go to sleeve - Closure from behind, connect two threads contra
Hold card give it to dr. - Release short thread from card, hold it going direction of anti-clockwise , then knot long thread after twirl maneuver
-
Gloves - after raising hand covering wrist -
- Open Bag from outside - RT & LT THUMB up roof- Wear inside out
- Put thumb to the roof same direction to opening
- RT traction then leave it dont pull - right hold from inside
- LT - pull completely, then pull RT from inside
- Fix both after completion
if given by nurse
- tell nurse right or left to start-
- put hand to direction to the glove from thumb
- then push in same direction
- take scrub from OR
- Head cap
- Face mask
- Gown
- Shoes cover
Dont touch anything blue/green - i.e. sterile instruments
Suturing
- Needle Holder - Ring finger w/ thumb
- Needle distal 1/3 to 2/3 & Straight 90 degree
- Movement - Supination + Pronation
Forceps - hold like pencil
CCTD 2 SK Nasogastric tube insertion
Nasogastric Tube & Enteral Feeding
Indications for GI Intubation
- To decompress the stomach and remove gas and fluid
- To lavage the stomach and remove ingested toxins
- To diagnose disorders of GI motility and other disorders
- To administer medications and feedings
- To treat an obstruction
- To compress a bleeding site
- To aspirate gastric contents for analysis
paralytic illeus, gastric lavage (suction) better in Double lumen Medication, nutrition (delivery)
contraindications
Absolute
- Facial trauma and/or basilar skull fracture
- Esophageal stricture
- Alkaline ingestion
Relative
- Coagulopathy
- Prior gastric surgery (e.g., gastric bypass)
- Recent nasal surgery
complications
- Clogged Tube- most common
- Oral mucosal breakdown
- Nasal irritation/ulceration
- Dumping Syndrome.
- Aspiration during feeding : ensure head of bed is elevated at least 30 degrees while feeds are being administered
- Dehydration- diarrhea is a common problem.
- Electrolyte imbalance: hyperkalemia and hypernatremia
- Gastric mucosa ulceration
Items
- nasogastric tube or (single lumen tube) or (laven) - can be used as suction and feeding - better for double lumen
- Double lumen tube (salim sump??) - better in suction due venting
confirm tube by x-ray from the blue lines in the nasogastric tube
Procedure
Exposure | position | privacy | Ask for vitals
- W ash hands (before and after)
- I ntroduce yourself to the patient and seek his or her consent
- P osition the patient correctly.
- E xpose the patient as needed (e.g. ‘Please take off your shirt for me now, if that is all right’)
- R ight side of the bed
ACTING - not i will do
greet amm ahmad, introduce your self, explain the procedure (reach nose to stomach for suctioning or medications), take permission, wash hands, close curtain, take nurse to assist, hand client glass water keep it in vicinity.
know reason why to put nasogastric tube - suction or delivery mainly?
ask patient previous nose administration, if he knows size of the nasogastric tube.
-
if theres any pain raise your left arm (OBTAIN SIGN) stop procedure.
-
Position 45 degrees - Position the patient in a semi-sitting or high fowlers position. If comatose-semi fowlers, expose upper trunk
-
take distance from nose to lobe behind ear, to side of neck, till the xiphoid process
-
Lubrication - best lidocaine appliance patient to his own nose
-
ask patient which nose is used previously -
-
inspect for most patent (septal defect, polyps, lesions) other way (close nose take breath check for most patent) - Emphasize the need to mouth breathe and swallow during the procedure
-
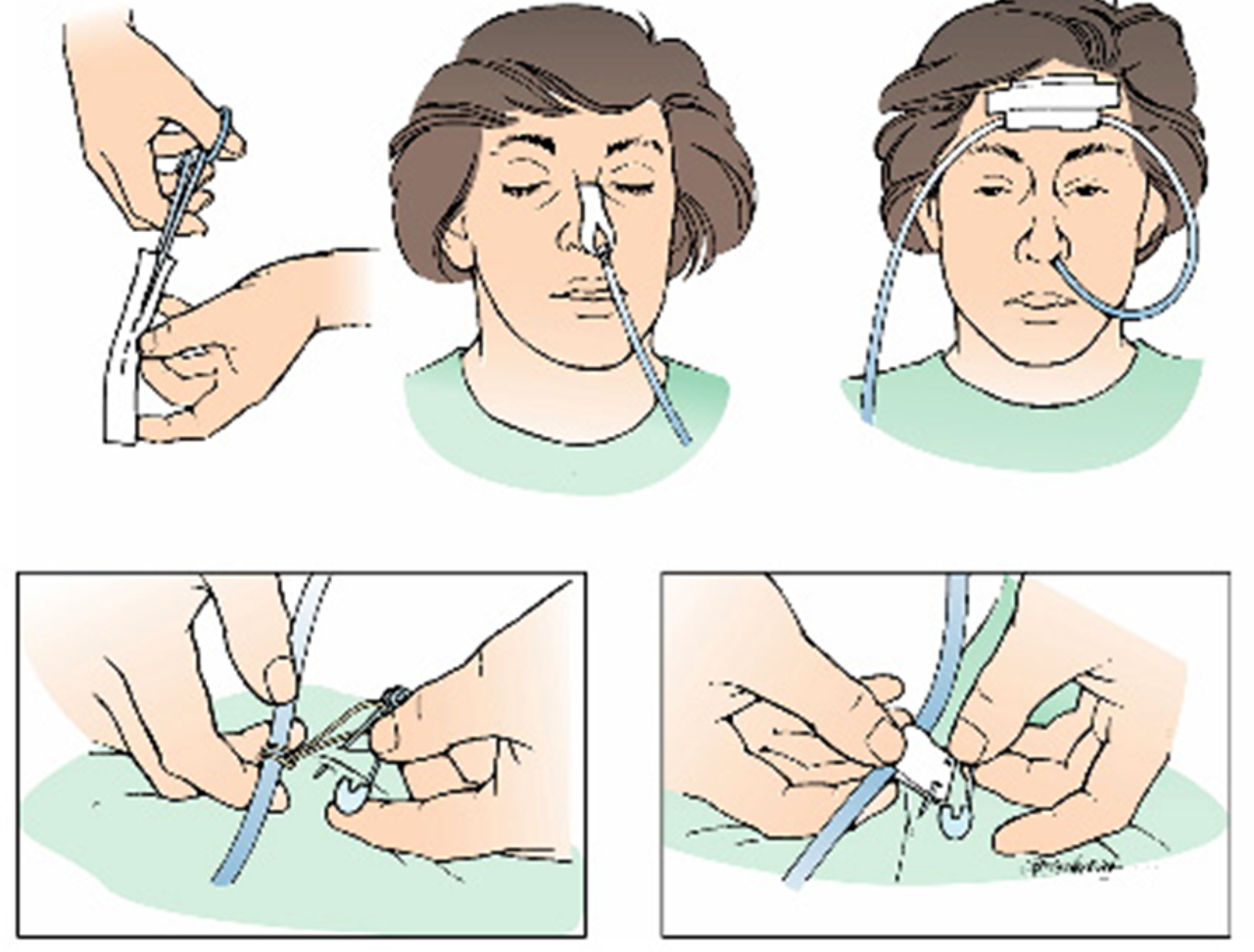
flexion of head whilist insertion - ask patient to swallow, Gently insert tube through nostril to back of throat (posterior naso pharynx). Have patient flex head toward chest after tube has passed through naso pharynx If resistance is met or client starts to cough, lacrimation, choke or become cyanotic stop advancing the tube and pull back.
-
Fix it - Secure the tube with tape or commercial device
-
Confirmation - check correct placement A) with suction (May not be accurate - may be no acid) (comment on food characteristics)
B) pH TEST - 5.5 ph in stomach normally with test pH automatic or strip - empty fluid in the field -
C) BUBBLES take the stethoscope heart the stomach, push air to listen for any bubbling in epigastrium
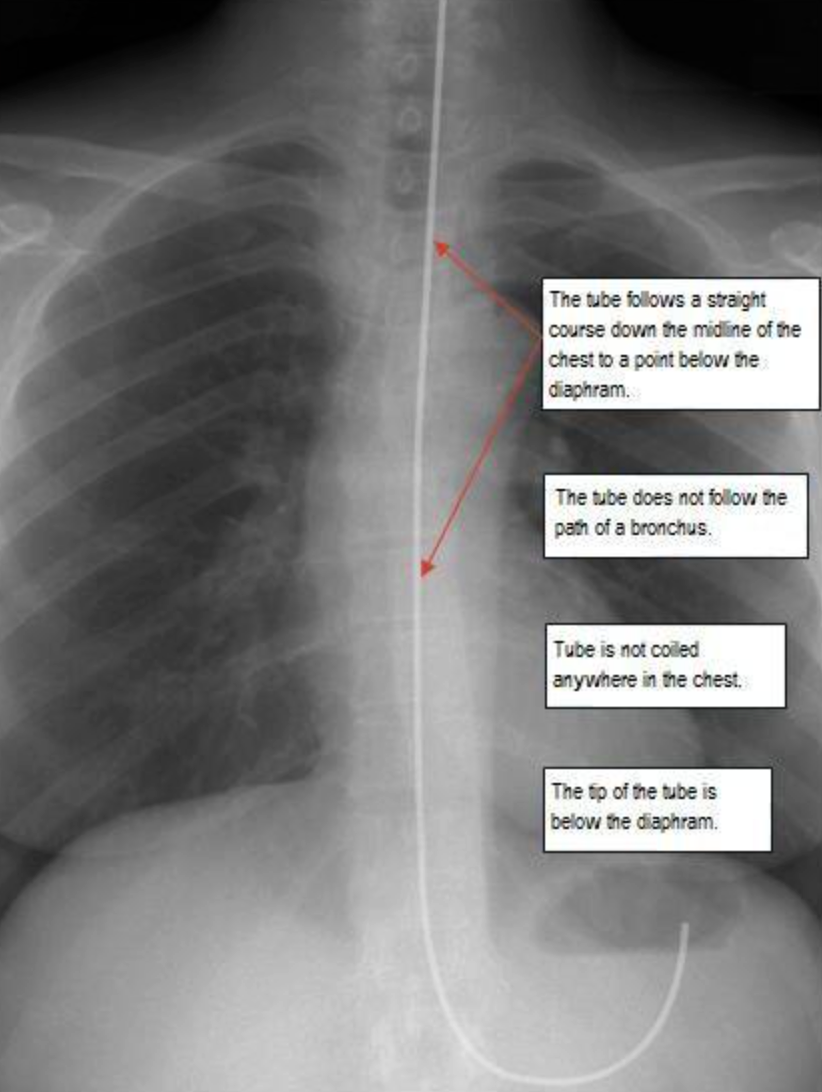
D) X-ray GOLD STANDARD to check - a tube passing center of chest, passing diaphragm, tip below tip of diaphgramgm ((THREE FINDINGS SHOULD BE PRESENT))
E) CAPNOGRAM - high reading of CO2 means the nasogastric tube could be in the lung
X-ray placement - Mention
1- follows straight course through midline to below diaphram
2- tube not follow bronchus path
3- not coiling
4- tip tube below diaphragm
Fix it
Intubating the patient with an NG tube
-
Assessment:
-
Who needs an NG:
- Surgical patients (bowel obstruction, Ileus, …)
- Ventilated patients
- Neuromuscular impairment .
- Patient with swallowing disorders (post CVA, …)
-
Assess patency of nares.
-
Assess patient medical history:
- Nosebleeds
- Nasal surgery
- Deviated septum
-
Anticoagulation therapy
-
Assess patients’ gag reflex.
-
Assess patient’s mental status.
-
Assess bowel sounds.
CCTD 3 Urethral Catheterization
Indication of Urinary Catheter insertion
A urinary catheter is used in many different situations:
- Decompression;
- BPH
- A urinary catheter may be inserted to drain the bladder before or during a surgical procedure, during recovery from a serious illness or injury, or to collect urine for testing
- A urinary catheter may be used for a person who is incontinent of urine, if the person has wounds or pressure ulcers that would be made worse by contact with urine
- A urinary catheter is necessary when a person is unable to urinate because of an obstruction in the urethra
Contraindication
-
Known or suspected urethral injury in case of pelvic fracture (absolute)
-
Signs to suspect urethral injury (blood at meatus , gross hematuria ,perineal hematoma ,high riding prostate gland) - (absolute contraindications)
-
Urethral stricture, recent urethral or bladder surgery (relative) Combative or uncooperative patient (relative)
Complications
- Urinary tract infection (UTI)
- Trauma to urethra & bladder
- Paraphimosis
- Undesirable catheter retention
Caring for a Person with an Indwelling Urinary Catheter
-
Indwelling urinary catheters are connected by a length of tubing to a urine drainage bag
-
The tubing is secured loosely to the person’s body near the insertion site using a catheter strap or adhesive tape
-
Securing the tubing to the person’s body prevents the catheter from being accidentally pulled out during repositioning
equipments - catheter tray
-
Gel
-
syringe (with distilled water - to inflate ballon of catheter - capacity in cath)
-
sponges
-
Cotton swaps
-
tape to anchor tubing
-
forceps
-
foley’s catheter (two way/indwelling) (12cm pedia - 16-18cm adults)
-
or three way catheter (continuous irrigation & drainage)
-
Sterile drainage tubing with collection bag
-
Bath blanket
Procedure
Exposure | position | privacy | Ask for vitals
- W ash hands (before and after)
- I ntroduce yourself to the patient and seek his or her consent, explain procedure
- P osition the patient correctly.
- E xpose the patient as needed (e.g. ‘Please take off your shirt for me now, if that is all right’)
- R ight side of the bed
In Males
-
Greet patient, explain full procedure, take confirmation, nurse
-
before starting make sure everything is prepared
-
Open instrument and make it ready for use
-
ready the catheter - bifidone - saline - gin
-
Supine for males. (position and exposure)
-
Wear sterile gloves
-
Apply Drape
-
Non dominant hand will hold the skin, labia/penis
-
Retract skin,
-
Take cotton with bifidone then clean meatus circular away from point to scrotum in circular motion, do not return to same area throw cotton, wear new gloves after first - take another one with same motion - repeat three times -
-
inject lidocaine intro penile urethra
-
Keep holding with you non-dominant hand
-
then inject lidocaine gel lubricant in urethra
-
with your right hand, hold folly’s catheter then pull 90 degree from non-dominant whilist holding penis - put the catheter fully inside.
-
you can add extra lidocaine to catheter; Then insert with nondominant hand keeping it completely straight, then push catheter all the way until end - in females until urine flows
-
Then drop your non domininant hand
-
Confirm urine is flowing before inflating the balloon
-
Inflate balloon, then pull catheter to hold it in place, then connect the bag, tape the cath from side.
-
We keep bag below patient
Document the patient file time, did procedure go perfectly?, is there any hematuria or complications?
In Females
- non dominant hand to hold
- then use cotton with your right hand to clean around and inside the labia
- If it goes inside vagina, then throw it out and change the catheter
- 5-7 cm insertion - then when you see urine come out - push it more 2 cm then inflate the balloon
- attach by side of thigh
- keeping the bag below the patient, by the side of the bed
CCTD 4 Per rectal/digital/protoscope
WIPER Introduce, explain, permission, chap, privacy, wash, gloves POSITION AND EXPOSURE
Position & Exposure
- PR is part of abdominal exam - Mid chest to Mid thigh
- SIM’s position / left lateral debicutus position
Inspection
first pull buttocks check any abnormality You know it is chronic if there is a abundant loose skin
Comments on
-
Upper Fissure on posterior lumbar side & Lower fissure is anterior
-
Fistula (opening) - due abscess formation of tract // many fistulas due crohn, TB, investigate more to the patient.
-
Hemorrhoids (piles)
- Piles are not palpable (only visible due to vein compressibility)
-
Abscess most common complication of abscess is fistula formation
-
warts
-
Discharge / Redness / Any change
Palpation
Tell the patient that you will introduce your finger, ask patient to relax (if not there will be severe pain)
-
apply gel to your finger then massage anus until relaxation by moving pulp of the finger on the anal canal
-
Introduce tip of finger - then ask patient to grip on finger to check on sphincter tone for intact sphincter (neurological problem, trauma) then enter and look for prostate lobes
-
Rotate 360 degree of finger while insertion and exertion - comment
- hemorrhoids visible only cant be palpated
- smooth granular?
- Pathologies? (pulops, tumors)
- Prostate The absence of sulcus is a sign of BPH (medial is mostly benign while lateral is malignant)
- Look your fingers afterward (blood, stool, pus, discharge - comment)
Do not remove gloves or scope before looking for blood and other materials
Protoscope
puborectalis muscle is normally contracted will cause flexion and bending of anal canal causing it to be inclined upwards against the umbilicus then view good while retraction of the scope
it has two parts - shaft & obturator
- lubricate
- relax the area for until sphincter is viable - go deep afterwards
- introduce anoscope straight toward the umbilicus, you will see polyps
- pull obturator afterwards never push forward otherwise complications wuill arise
- take good view while pulling to see any polyps, discharges etc…
check protoscope for any abnormality
End
ask if patient needs any help, thank the patient document in patient files
CCTD Counseling - Breaking Bad News
Diagnosis for example: Nevus Melanoma - Biopsy Positive for Cancer
Be Sensitive - Show Empathy, Not Sympathy
- It’s important to express empathy sincerely. Avoid overdoing it or sounding rehearsed. For instance, say, “I’m sorry to have to share this news,” and offer appropriate physical comfort or support if necessary (like a hand on the shoulder). Keep a professional yet compassionate tone.
How to Break Bad News
-
Greet the Patient
- Introduce yourself and explain your role.
- Begin with a gentle explanation of the procedure conducted (e.g., “We performed a biopsy to gather more information regarding your condition…”).
-
Set a Supportive Environment
- Sit at the patient’s level, preferably at a right angle without a table between you to promote a feeling of openness. Lean slightly forward to show attentiveness.
- If they are alone, ask whether they would like family members or loved ones to join them for support before proceeding.
-
Explain the Findings
- Briefly summarize the patient’s medical history and the findings from the biopsy.
- Ask them if they have any questions, thoughts or concerns about their illness, to gauge their understanding and feelings.
-
Present the Result
- Be clear but sensitive when delivering the news of cancer: “The results confirm that the lesion we tested is melanoma, a type of skin cancer.”
Giving a “Warning Shot”
- Transition Thoughtfully: Before revealing the final diagnosis, give the patient time to mentally prepare (a brief “warning shot”). For example, “The tests showed something concerning” or “I have some news that may be difficult to hear.”
- Avoid Medical Jargon: Clearly explain in layman’s terms what melanoma is and how it can typically progress.
- Ask for Consent to Proceed: Allow them the option to pause or invite questions before continuing, saying, “Would you like me to explain the next steps?”
Avoid Premature Reassurance
- Avoid Offering False Hope: Give realistic answers such as, “We don’t have all the answers yet, but we’ll do everything we can to help.” Refrain from saying things like “everything will be fine” or providing absolute assurances.
- Use phrases like, “We are still in the process of understanding the full extent,” and acknowledge that “Only further tests and time will clarify all the details.” كل صغيره / علم عند الله
Explain Next Steps and Procedures
- Clearly outline immediate and future medical steps. For example:
- Biopsy findings.
- The option of excision to remove the melanoma.
- Potential treatments such as chemotherapy or immunotherapy if the cancer has spread.
- Reinforce that additional investigations may be needed before proceeding with a definitive treatment plan.
Signposting Treatment Options
-
Explain treatment choices in simple terms, and offer the patient a sense of agency over their decisions:
- “There are different treatment options we can explore, such as surgery to remove the melanoma, medication, or chemotherapy, depending on the extent of the spread.”
- Keep the patient informed of every step moving forward, using language like, “We’ll walk through each option together and make sure you understand fully before any decisions are made.”
-
Offer Ongoing Support: Express your commitment to helping them through the process: “I’ll be with you every step of the way.”
Breaking Bad News to Older Patients
If appropriate, discuss the diagnosis in a way that can ease later planning, such as treatment preferences, end-of-life care discussions, will preparation, or other long-term considerations, especially if the patient prefers to plan ahead.