Benign glandular and stromal hyperplasia of the transitional zone of the prostate Typically there is an increase in volume of the prostate with a calculated volume exceeding 30cc .
Post-micturition residual volume is typically elevated: More than 50 mL is usually considered abnormal.
Clinical presentation:
- To remember the symptoms of BPH, think “FUNWISE”: Frequency, Urgency, Nocturia, Weak stream /hesitancy, Intermittent stream, Straining to urinate, and Emptying (not emptying completely, terminal dribbling).
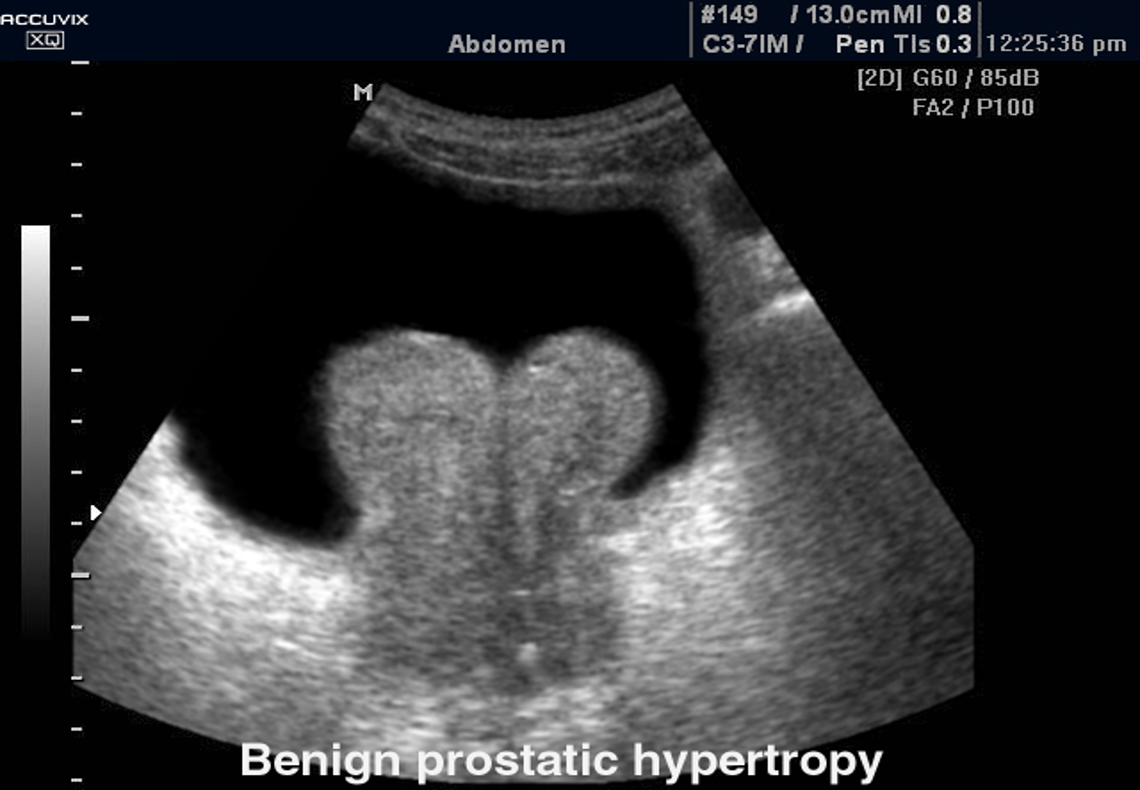
Ultrasound : Transabdominal ultrasound (TAUS)
Indications: Ultrasound pelvis: Consider prior to initiating treatment to assess the size of the prostate.
Supportive findings of BPH:
- Increased total prostate volume
- Elevated PVR volume
- Evidence of bladder outlet obstruction (e.g., bladder wall thickening and hydronephrosis ).
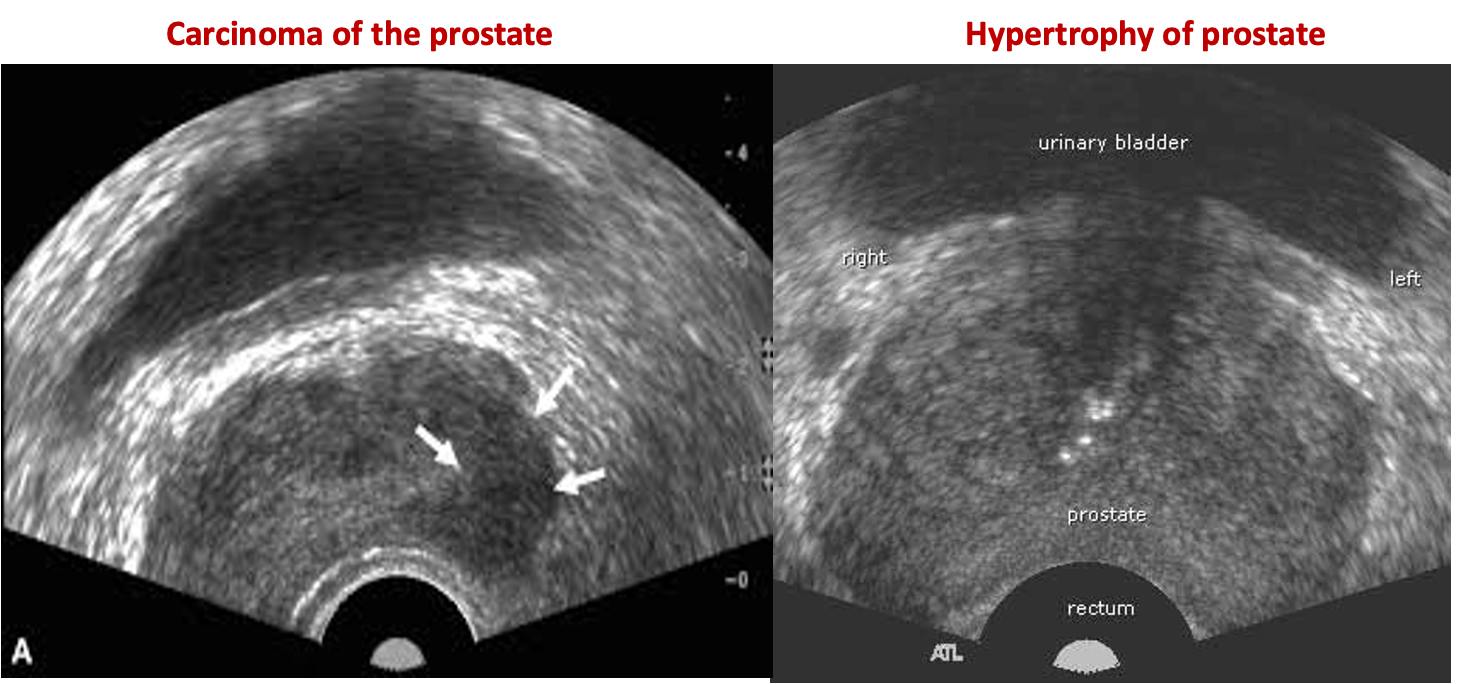
Transrectal ultrasound (TRUS):
TRUS is not required for the initial evaluation of BPH.
Indications
- Suspected prostate cancer to guide biopsy
Case . 75 years old male with retention of urine
Transrectal ultrasound images of prostate
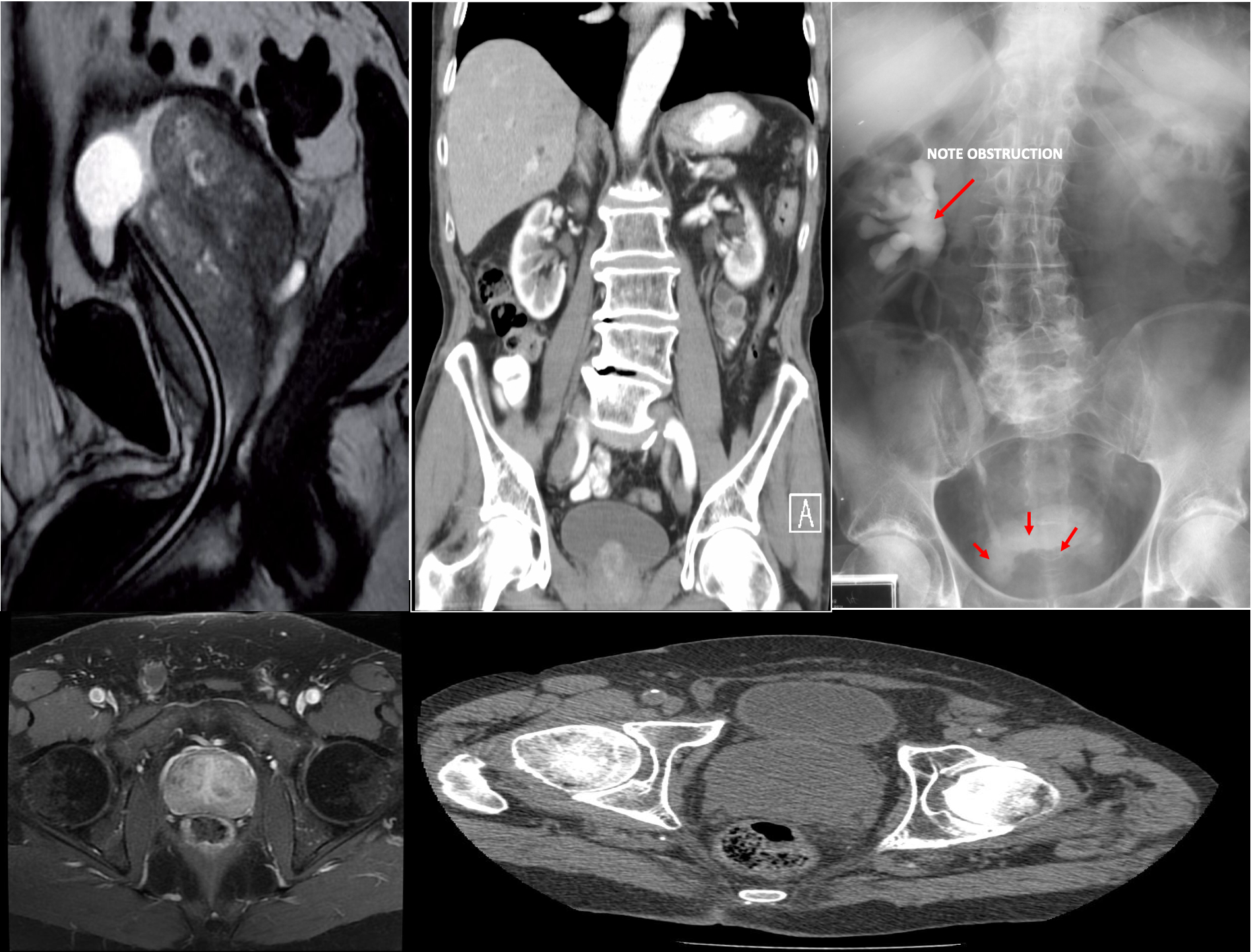
MRI and CT pelvis
-
Commonly used for preprocedural assessment of prostate volume and localization of enlarged tissue
-
MRI can potentially differentiate BPH from prostate cancer.
Enlarged prostate gland - MRI pelvis (T2-weighted, sagittal plane) The enlarged prostate gland is lobulated and heterogeneous. The bladder base is elevated. A foley catheter is in place.
This can obstruct the ureters entering the bladder leading to hydronephrosis and renal failure.
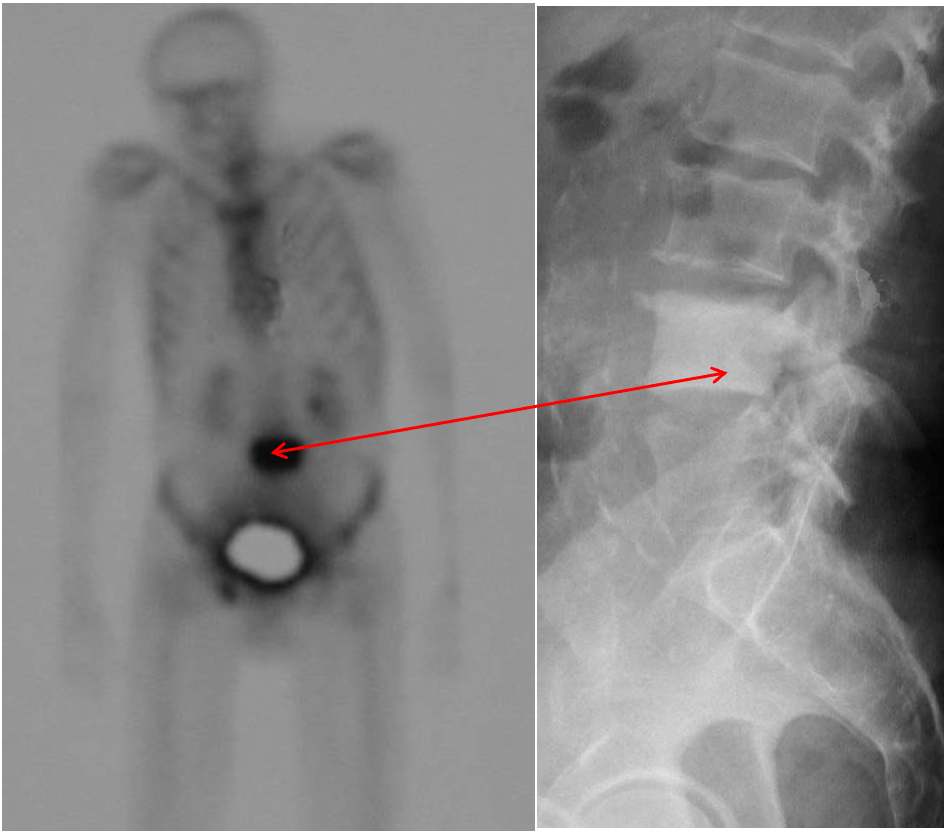
The nuclear bone scan
shows increased activity at site. Prostate malignancy often metastasizes to the skeleton and is usually sclerotic (dense) .