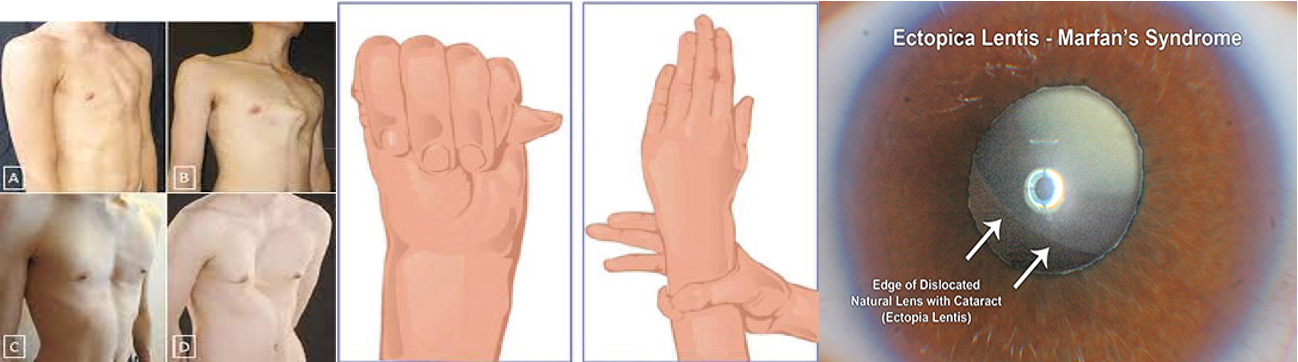
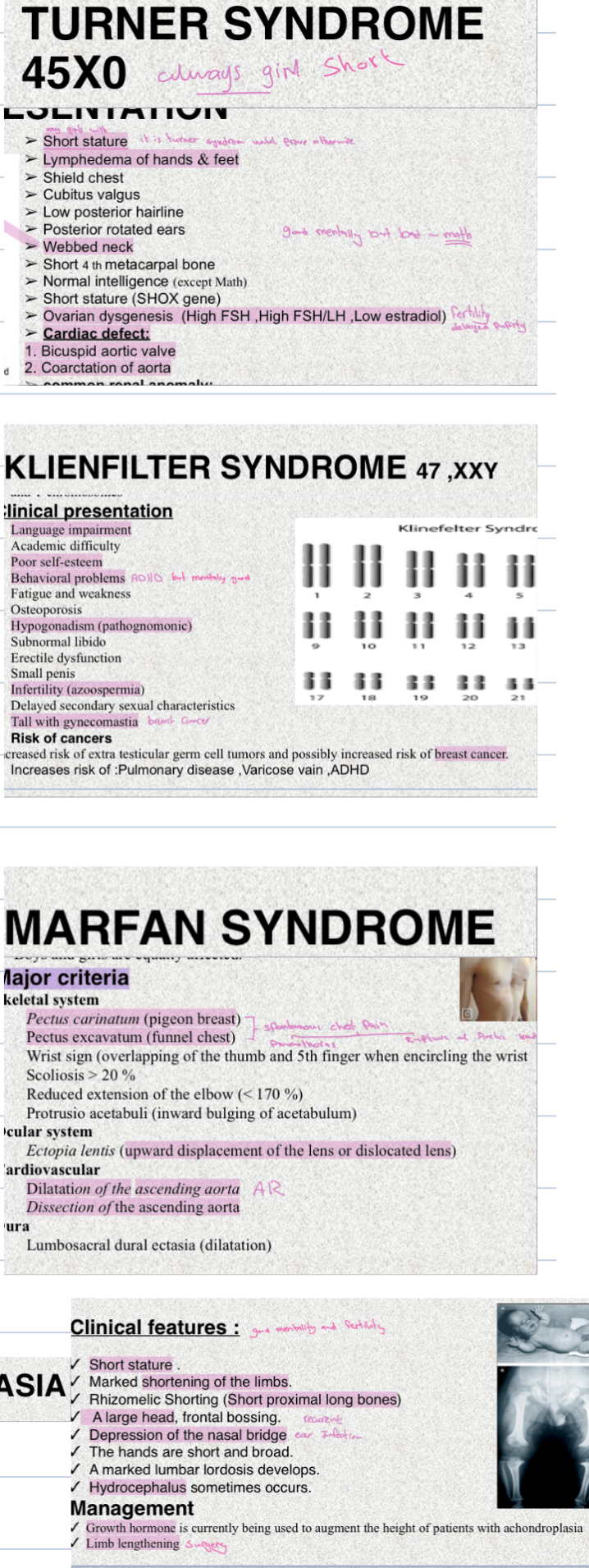
Marfan Syndrome
Girl presented with tall stature, long arms. What is the diagnosis?
- Heritable genetic defect of connective tissue
- Autosomal dominant mode of transmission
- Boys and girls are equally affected
Major Criteria
Skeletal System
- Pectus carinatum (pigeon breast)
- Pectus excavatum (funnel chest)
- Wrist sign (overlapping of the thumb and 5th finger when encircling the wrist)
- Scoliosis > 20%
- Reduced extension of the elbow (< 170%)
- Protrusio acetabuli (inward bulging of acetabulum)
Ocular System
- Ectopia lentis (upward displacement of the lens or dislocated lens)
Cardiovascular Z
- Dilatation of the ascending aorta
- Dissection of the ascending aorta
Dura
- Lumbosacral dural ectasia (dilatation)
Minor Criteria
Skeletal
- High arched palate
- Moderate pectus excavatum
- Joint hypermobility
Cardiovascular
- Mitral valve prolapse
Pulmonary
- Dilatation of the main pulmonary artery
- Spontaneous pneumothorax
- Apical blebs
Skin
- Striae atrophicae
- Recurrent incisional hernias
18-Day-Old Girl with Down Syndrome - Refusal to Feed
-
An 18-day-old girl with Down Syndrome presents to the clinic with a complaint of refusing to feed. She is also noted to be tachypneic and tachycardic. On examination, she has a 2nd-grade murmur.
-
Two relevant questions:
- Is she experiencing sweating with feeding or cyanosis?
- Is there any edema present?
-
What findings will you look for on examination?
- Detailed assessment of the murmur (location, intensity, radiation).
- Signs of heart failure (e.g., hepatomegaly, respiratory distress).
- Peripheral pulses and capillary refill.
- Signs of cyanosis (central or peripheral).
- Presence of edema.
- Respiratory rate and effort.
- General assessment for other features of Down Syndrome.
-
Mostly diagnosis?
- The most likely diagnosis, given the clinical picture, is a congenital heart defect, specifically Atrioventricular Septal Defect (AVSD), which is the most common cardiovascular anomaly in Down Syndrome.
-
What is your management plan?
- Initial Management:
- Stabilize the patient: Ensure adequate oxygenation and ventilation.
- Start on diuretics (e.g., Lasix) to manage fluid overload.
- Initiate an ACE inhibitor (e.g., captopril) to reduce afterload.
- Monitor vital signs closely.
- Further Investigations:
- Echocardiogram to confirm the diagnosis and assess the severity of the defect.
- Chest X-ray to evaluate for cardiomegaly and pulmonary edema.
- ECG to assess for any rhythm abnormalities.
- Thyroid hormone levels to assess for hypothyroidism, which is common in Down Syndrome.
- Definitive Management:
- Cardiac surgery to repair the AVSD. The timing of surgery will depend on the severity of the defect and the patient’s clinical condition.
- Nutritional support: Address feeding difficulties with appropriate strategies.
- Ongoing monitoring and follow-up with a cardiologist.
- Initial Management:
Down Syndrome Patient
- Picture: (Image of a Down Syndrome patient is assumed here)
- What is the most common cause of this syndrome?
- (Nondisjunction)
- Which of these investigations help you in assessing this patient?
- (Thyroid hormone levels)
- What is the most common cause of this syndrome?
Case
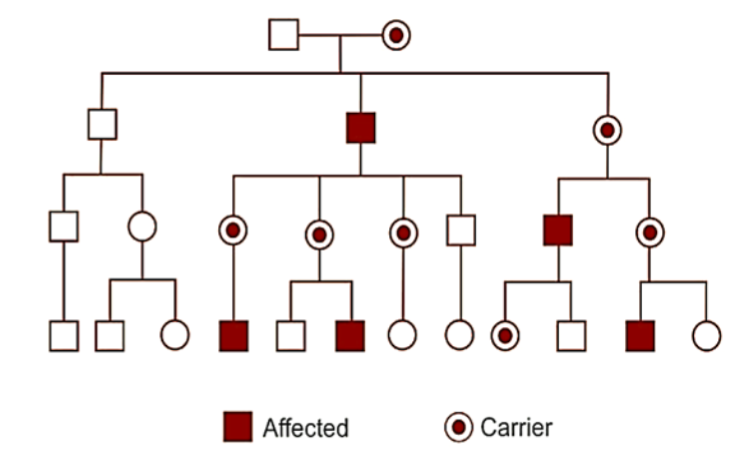
1. Name the mode of inheritance? X-linked Recessive 2.What are the features seen on a family tree? males affected exclusively, the gene alteration is transmitted from female carriers to sons, affected males cannot transmit the condition to their sons. 3. Mention 1 example ? Hemophilia, Duchenne’smuscular dystrophy, G6PD deficiency, Albinism

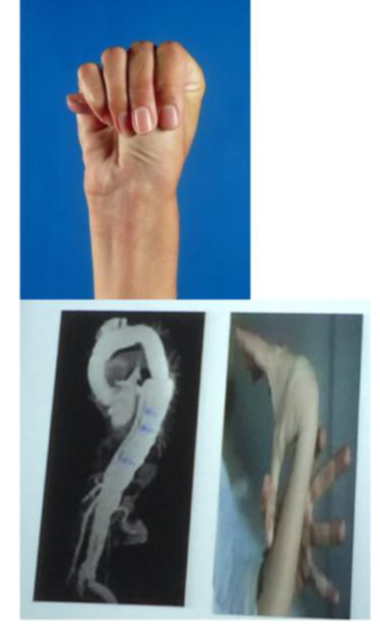
Diagnosis: marfan Syndrome. Describe? * Aortic dissection * Lax joints
-
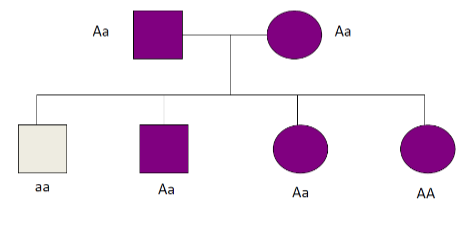
What is the inheritance in this pedigree? Autosomal dominant pedigree.
-
Examples? Marfan syndrome, Osteogenic imperfecta, Porphyria, Achondroplasia

Prader Willi Syndrome
- Symptoms? Polyphagia, mental retardation, obesity, and short stature.
- Diagnosis? Prader-Willi syndrome.
 Q2A-B
Q2-A: What’s most likely the diagnosis? Or the cause of this appearance?
A: Cephalhematoma Bilateral
Q2-B: What’s might be the complications?
A:
Q2A-B
Q2-A: What’s most likely the diagnosis? Or the cause of this appearance?
A: Cephalhematoma Bilateral
Q2-B: What’s might be the complications?
A:
- Anemia
- Infection
- Hyperbilirubinemia
 Q3A-B This patient came with high serum calcium and supravalvular aortic stenosis. Z
Q3-A: Most likely the diagnosis?
A: Williams syndrome.
Q3-B: What’s the cardiac lesion related to this case?
A: Aortic stenosis.
Q3A-B This patient came with high serum calcium and supravalvular aortic stenosis. Z
Q3-A: Most likely the diagnosis?
A: Williams syndrome.
Q3-B: What’s the cardiac lesion related to this case?
A: Aortic stenosis.
Z
 Name the disease?
Erb’s palsy showing the typical ‘waiter’s tip’ position of the hand. Note the Asymmetric unilateral moro reflex on the left
Name the disease?
Erb’s palsy showing the typical ‘waiter’s tip’ position of the hand. Note the Asymmetric unilateral moro reflex on the left
Name the location of disorder? C5, C6**




 What does the picture show? Brushfield spots, single palmar crease
What does the picture show? Brushfield spots, single palmar crease
Name the disease Down syndrome Associated cardiac defects? VSD,AVSD
Eight-year-old girl with dysmorphic features and learning disability. She was operated for congenital heart disease at infancy.
Describe facial features? Round face. Flat nasal bridge .-. Small mouth. protruding tongue - small ear -upslanted palpebral fissure…
What is the most common Musculoskeletal Problems? Atlantoaxial instability
What is the most common endocrine complication? * Hypothyroidism
What are the long-term complications associated with Down Syndrome? Leukemia, hypothyroidism, and obesity.
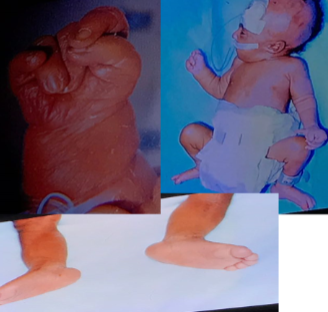


Congenital Heart Disease and Dysmorphic Features:
- Newborn with dysmorphic features and congenital heart disease.
- Q2. Which of the following is likely associated with this syndrome?
- a. Ventricular septal defect
- b. Complete atrioventricular septal defect
- c. Pulmonary stenosis
- d. Coarctation of the aorta
- Q2. Which of the following is likely associated with this syndrome?
- a. Down’s syndrome
- b. Edward’s syndrome
- c. William’s syndrome
- d. Turner syndrome
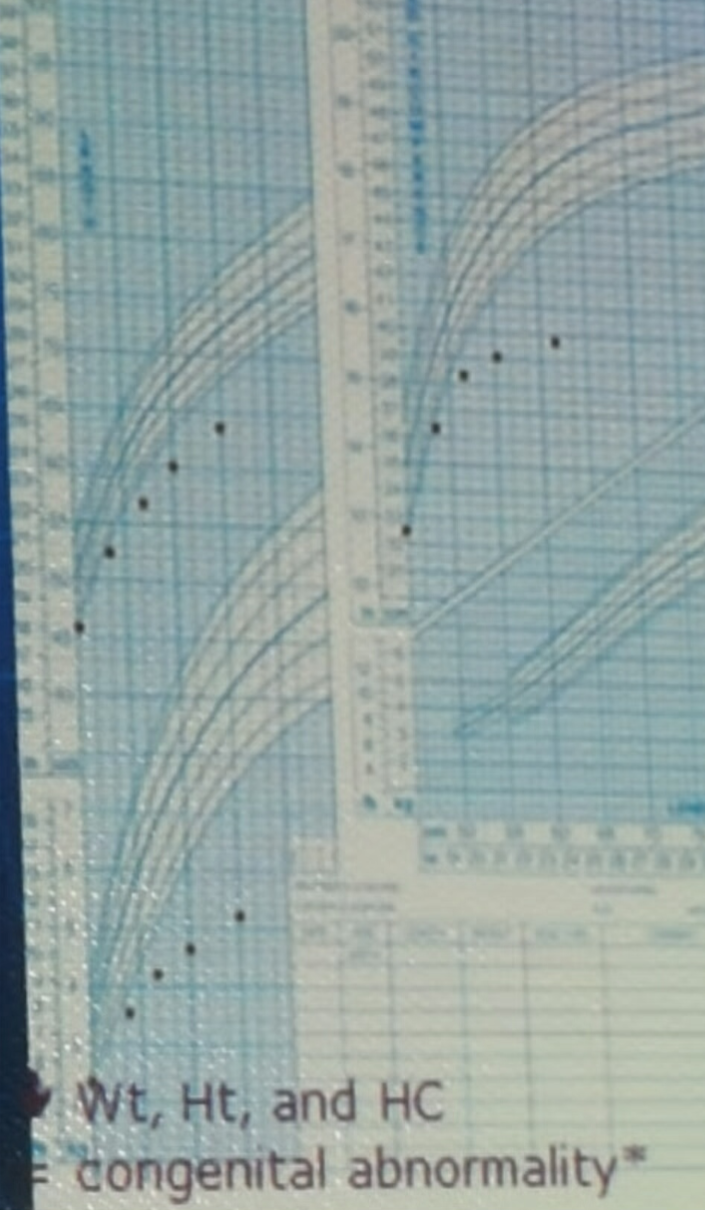
What is observed in the growth chart? All parameters (weight, height, and head circumference) are under the 3rd centile and worsening over time.
What is the likely diagnosis? Mostly a genetic syndrome, such as Edward Syndrome.
Z
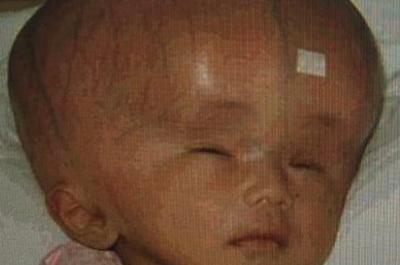

 3 months old boy presented to ER
3 months old boy presented to ER
- Name three abnormalities you see in the picture?
- Large head macrocephaly
- Frontal bossing
- Dilated veins
- **Sunset eyes()
- What is the diagnosis? Hydrocephalus..
- What is the treatment? VP shunt - Treat the underlying Cause..
INvestigations Urgent brain ct scan
What are the possible diagnoses based on the clinical presentation? Familial hydrocephalus, cerebral gigantism, or pseudo-syndrome.
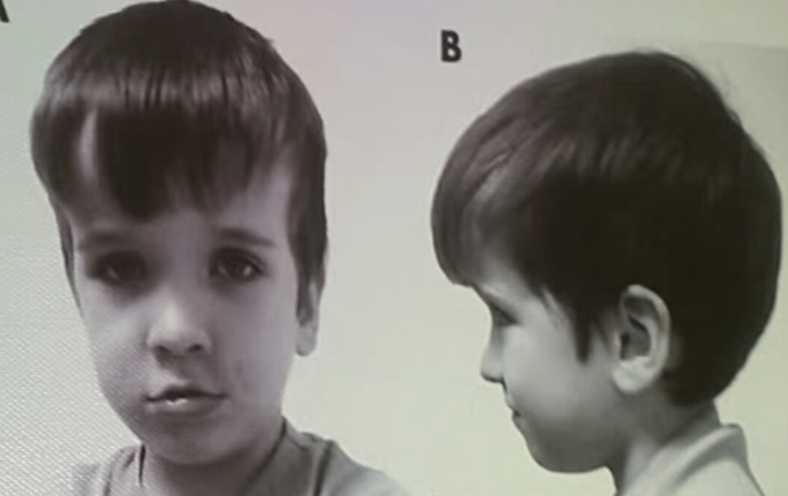
Oxycephaly / Tower shape head (scaphocephaly)??
What are the clinical features? Frontal bossing and increased AP diameter. What are the possible diagnoses? Familial, premature, or Apert syndrome, Rickets or thalassemia frontal bossing

Oblique Cephalus
What is observed in the clinical presentation? Oblique head shape. What are the possible diagnoses? Familial, Crouzon syndrome, or Caput.

Diagnosis: Bilateral cephalohematomas
- Cause? Instrumental delivery or birth injury
- Complication? Anemia, Hyperbilirubinemia, Infection
Case Study
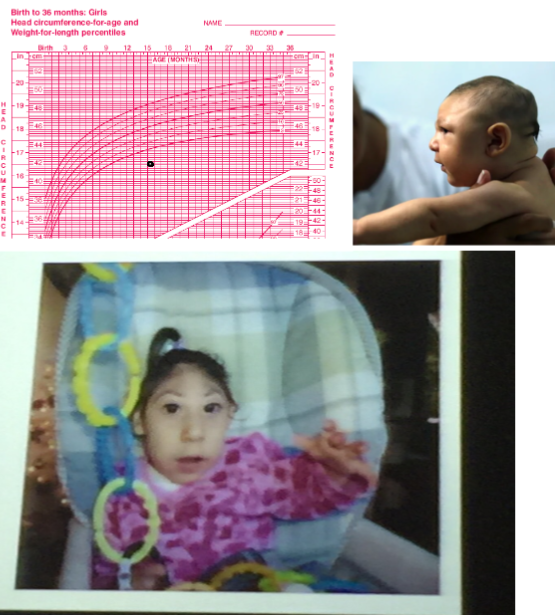
Questions
- Head circumference Growth Chart of 15 months old Brazilian girl, her mother was febrile and had skin rash during pregnancy. Q1. What is the abnormal finding in the growth chart?
- Microcephaly (head circumference below the 3rd centile)
- Q2. What is the likely cause of the abnormal finding in the growth chart?
- Zika virus, Trisomy 13, 18, and 21, Familial microcephaly, Post meningitis, Post intracranial hemorrhage
What are the possible diagnoses based on the clinical presentation? Familial microcephaly or TORCH infection.
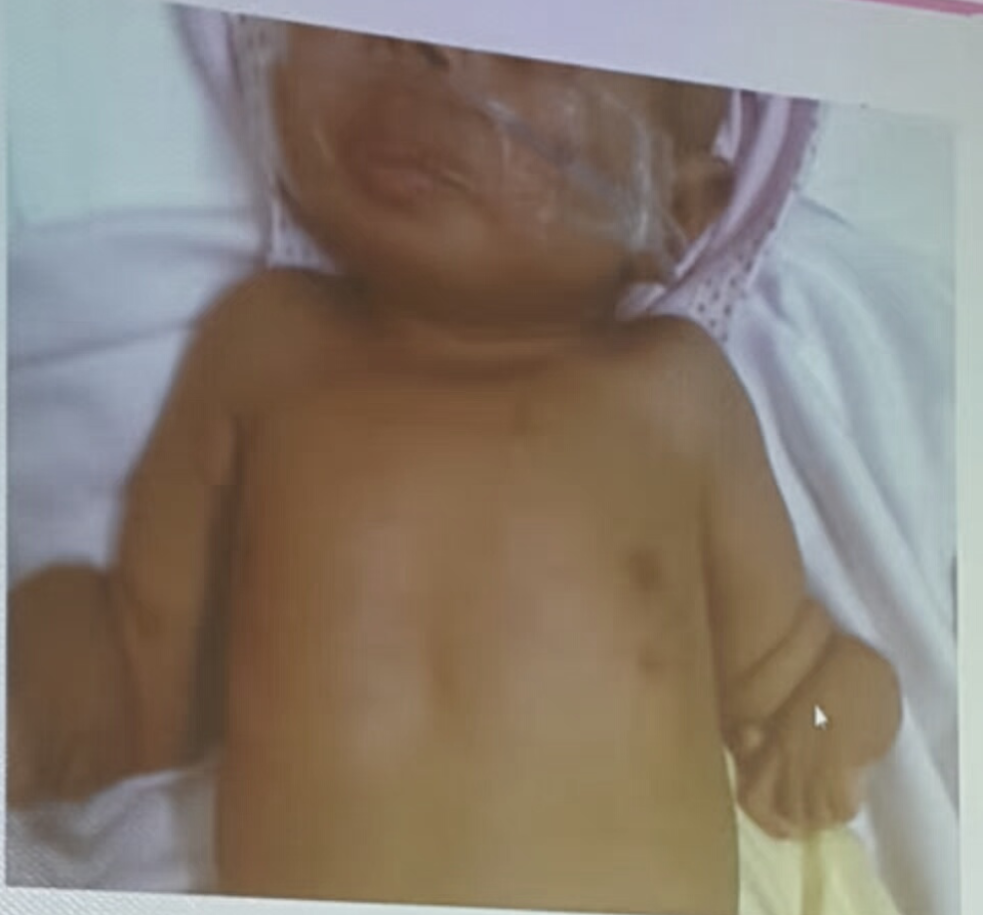
Case Study: ambiguous genitalia

Questions
- A-Give one sign?
- According to doc. Not the one in senario (hypotensive and dehydration sign was mention) or the picture?
- It could be hyperpigmentation
- B-give one electrolyte abnormality?
- Hyperkalemia, hyponatremia
- C- what is the most likely enzyme to be deficient?
- 21-hydroxylase
- D- the most important medication to give?
- Cortisone
Case Study: Hypoxic-Ischemic Encephalopathy (HIE)

Questions
- A 10 month suffered from moderate to severe HIE which he recovered from, He shows spastic posture, what is the diagnosis?
- Rt facial palsy LMN
Case Study 48: Holt-Oram Syndrome & Trisomy 13 (Patau Syndrome)

Case Study 49: Turner Syndrome, Klinefelter Syndrome, Marfan Syndrome, Achondroplasia

 What are the clinical features? Foot edema (non-pitting), low set hair, webbing of the neck, and deformed ear.
What are the clinical features? Foot edema (non-pitting), low set hair, webbing of the neck, and deformed ear.
What are the associated complications? Aortic coarctation and pulmonary stenosis.
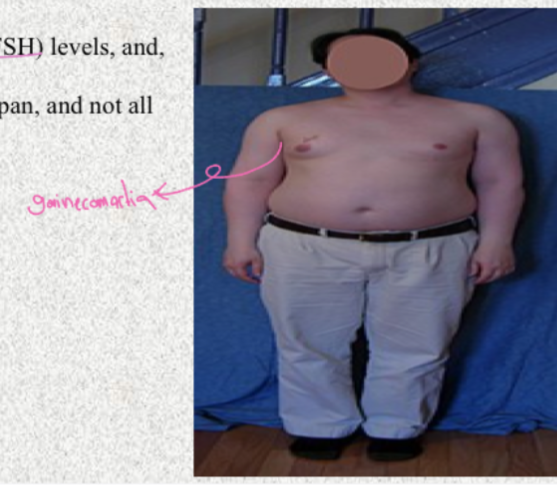
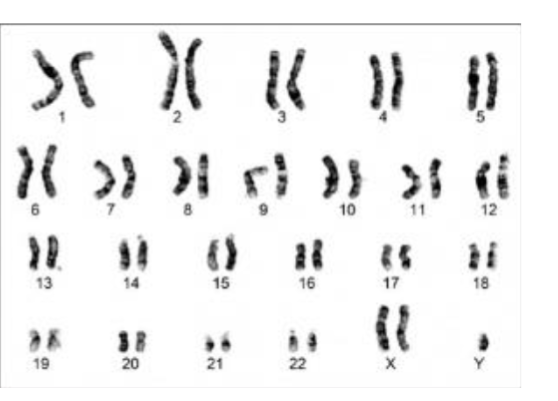
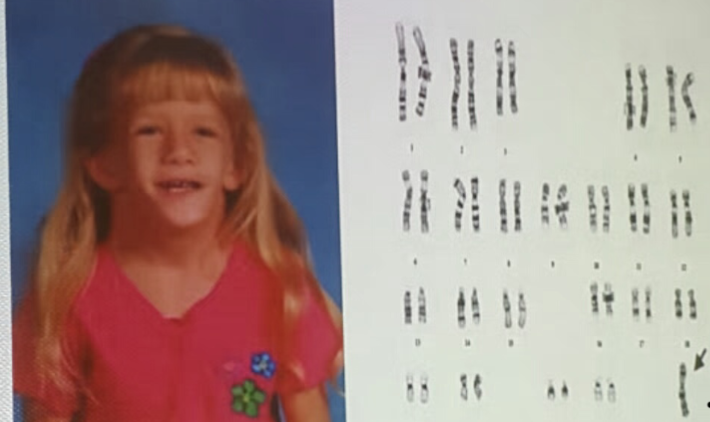
Case
The karyotype shown is for a child with tall stature and learning disability. What is your diagnosis? Klinefelter syndrome




Turner Syndrome (XO)
• Patient with webbed neck And hand leg swelling • Diagnosis ? • Turner syndrome • Associated heart disease ? • CoA
- Describe? Bilateral foot edema.
- Confirm by? Chromosomal analysis.

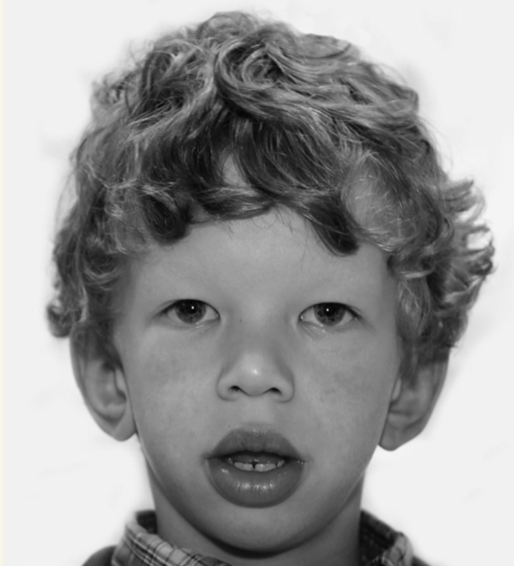
Diagnosis: Williams syndrome
- Dysmorphic feature? Flattened nasal bridge, puffiness around the eye, no epicanthal fold, large upper lip
- Associated cardiac disease? Aortic stenosis

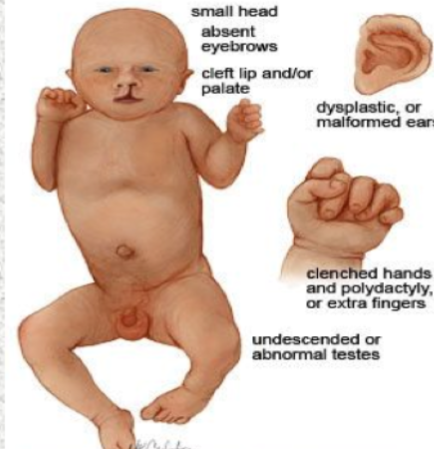
Describe
- Cleft lip and palate
- Clinched hand with polydactyly
- Diagnosis? Patau trisomy 13

Sturge-Weber Syndrome Z
What is the likely diagnosis? Neurocutaneous syndrome, specifically Sturge-Weber syndrome.
What type of seizure is associated? Partial seizures.

Diagnosis: Plagiocephaly Z
- Cause? Prolonged pressure on the same area
- Treatment? Physical therapy

- A 12-year-old girl has had recurrent episodes of swelling of her hand and feet for the last 6 months. These episodes occur following exercise and emotional stress, last for 2-3 days, and resolve spontaneously. The last episode was accompanied by abdominal pain, vomiting, and diarrhea. The results of routine laboratory workup are normal. An older sister and a maternal uncle have had similar episodes as shown in the photographs below. Hereditary Angioedema