Y ?
Failure to Thrive
Overview
Failure to Thrive (FTT) is a condition characterized by abnormal weight status during the infant-toddler years and/or abnormal weight gain, specifically in terms of weight growth velocity.
Abnormal Weight Status
Abnormal weight status is referenced against:
- Genetic growth expectations for the family.
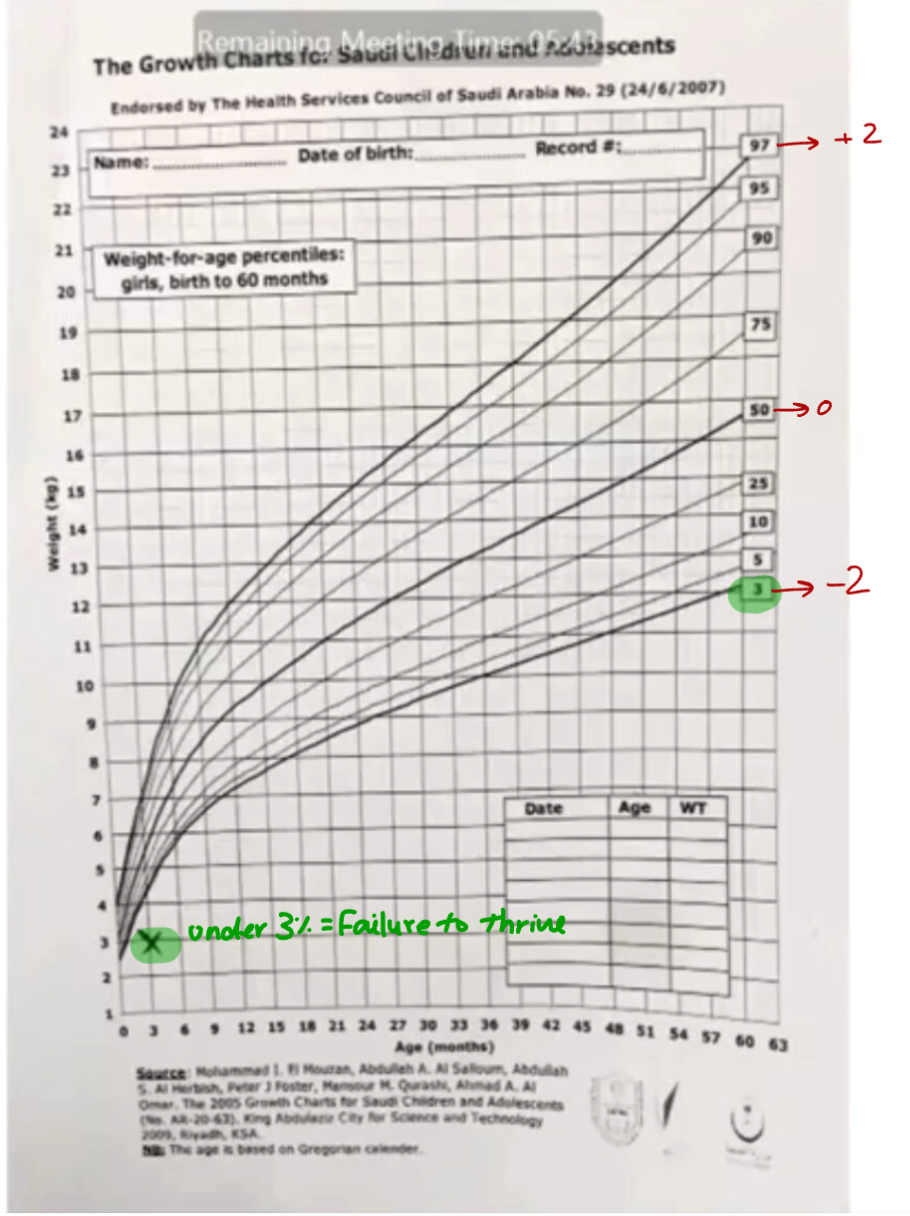
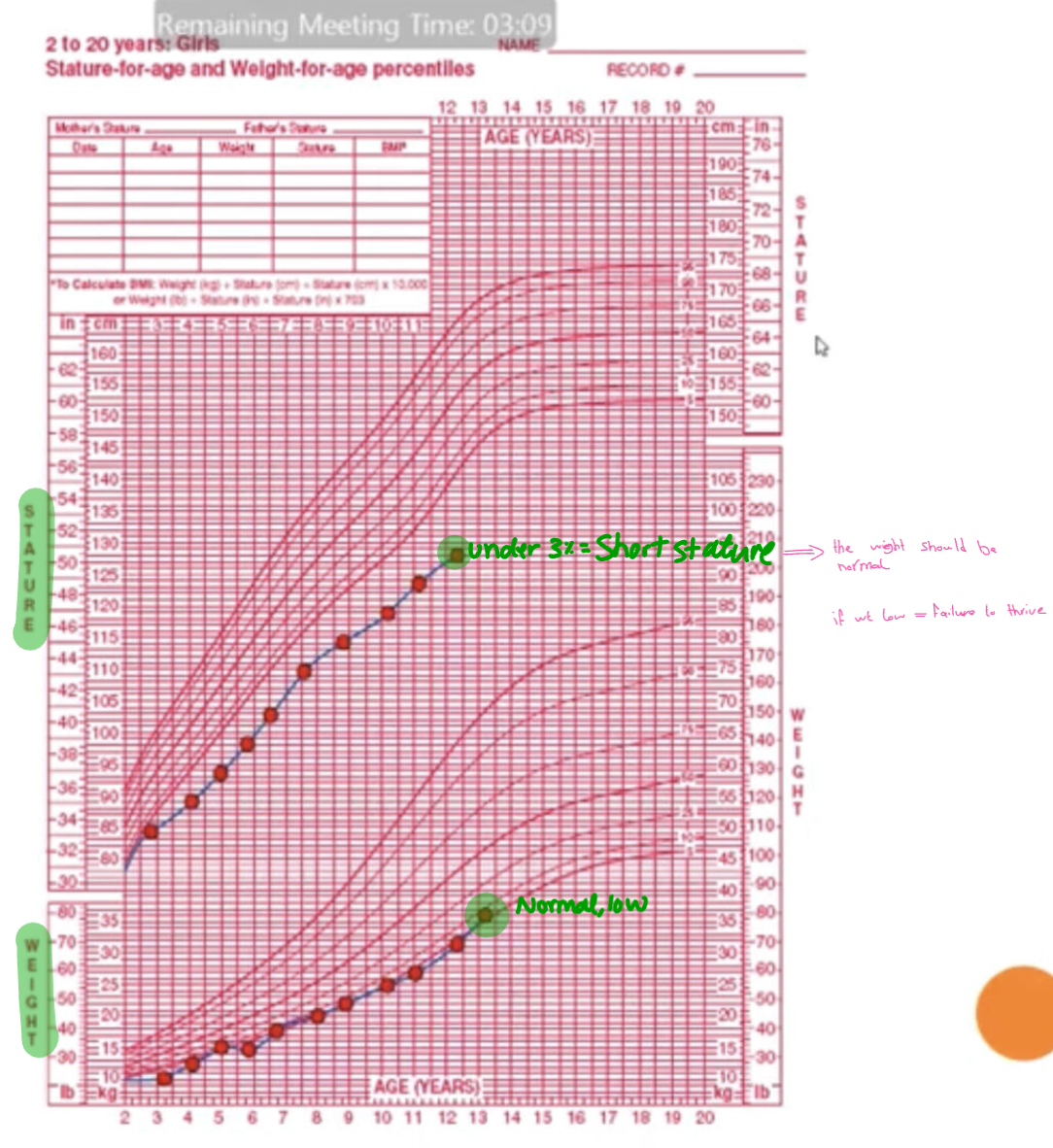
- Children of the same gender and gestation-adjusted age, particularly those below the 3rd percentile on growth curves.
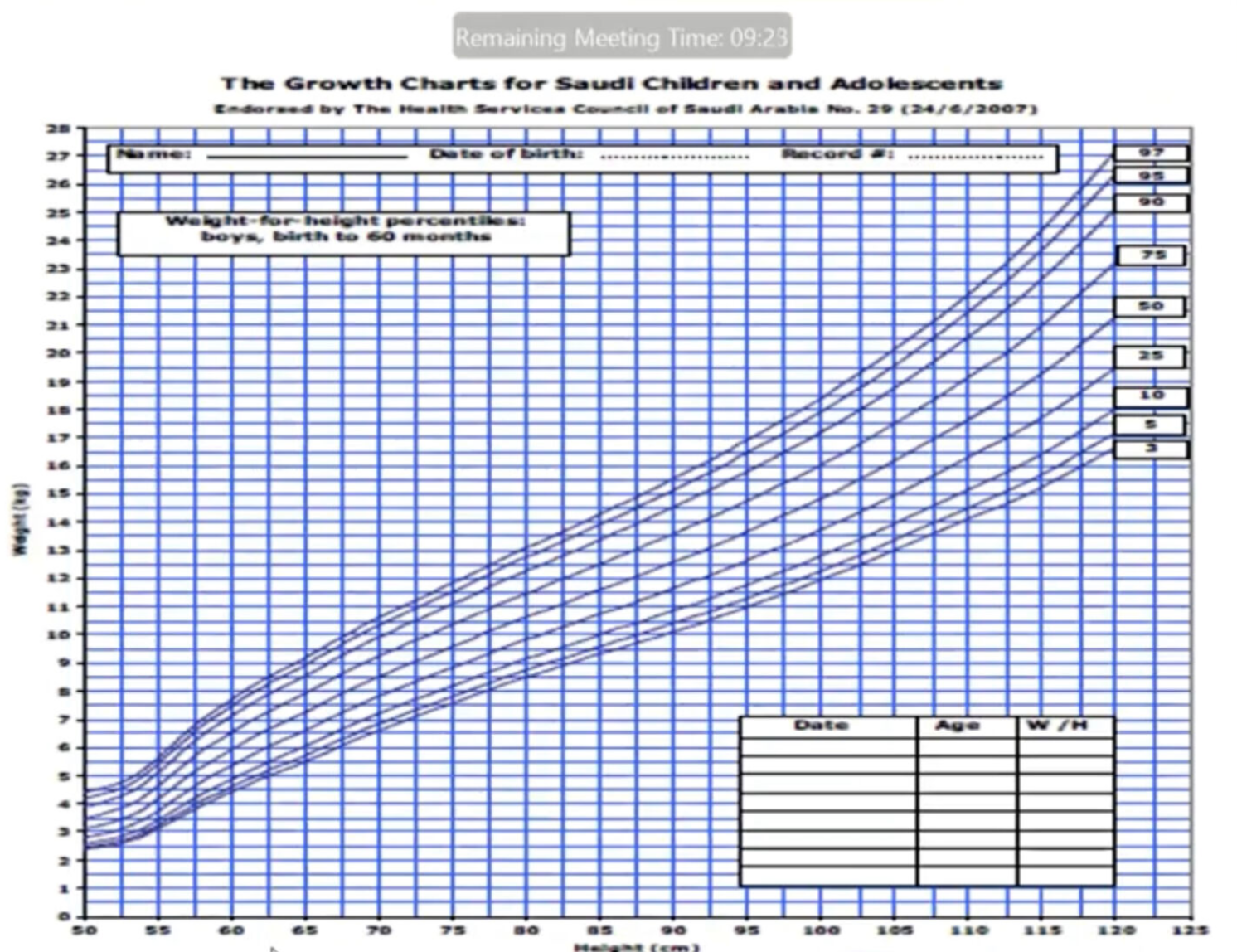
- The child’s own length, particularly if below the 10th to 25th percentile on growth curves.
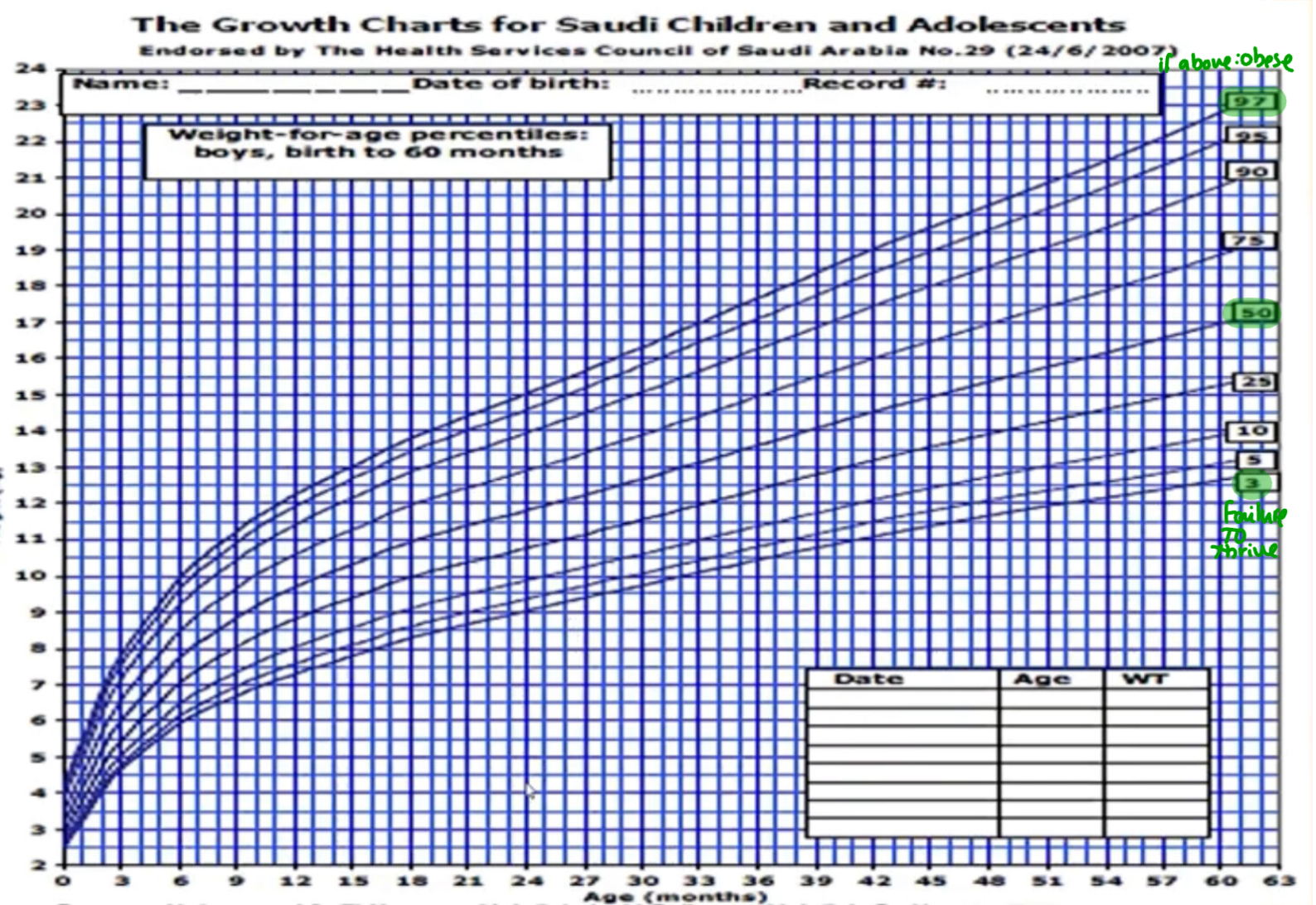
Growth Charts
The growth charts for Saudi children and adolescents are endorsed by The Health Services Council of Saudi Arabia. These charts are essential tools for assessing growth patterns and identifying potential cases of FTT.
Abnormal Weight Gain (Growth Velocity)
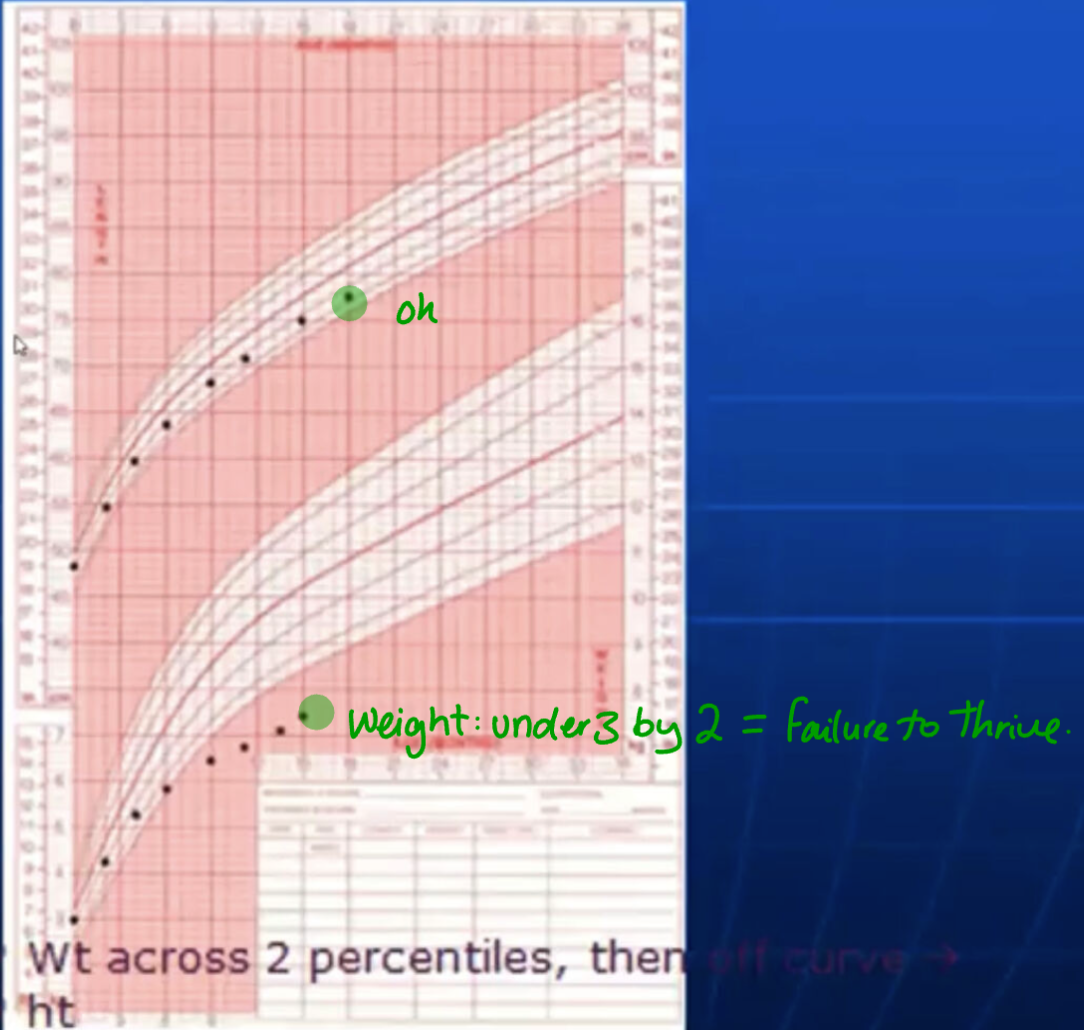
- Falling across two standard deviation percentile lines on growth curves over a six-month period.
- This should be observed for at least one to two months.
Definition of Failure to Thrive
- Weight is abnormally two standard deviations below the mean for gestation-corrected age.
- Weight crosses percentile curves by two standard deviations.
- The weight-to-height ratio is depressed.
Genetic Factors Y
- Children may be genetically small due to the size of their parents.
- Children born small for gestational age (SGA) may never catch up.
- If born larger than normal, long-term genetic potential may demonstrate a decreased growth rate in the first two years.
Growth Only Y
- FTT is not necessarily associated with developmental or emotional problems in the child.
- It is not necessarily caused by environmental factors.
Long Duration FTT Y
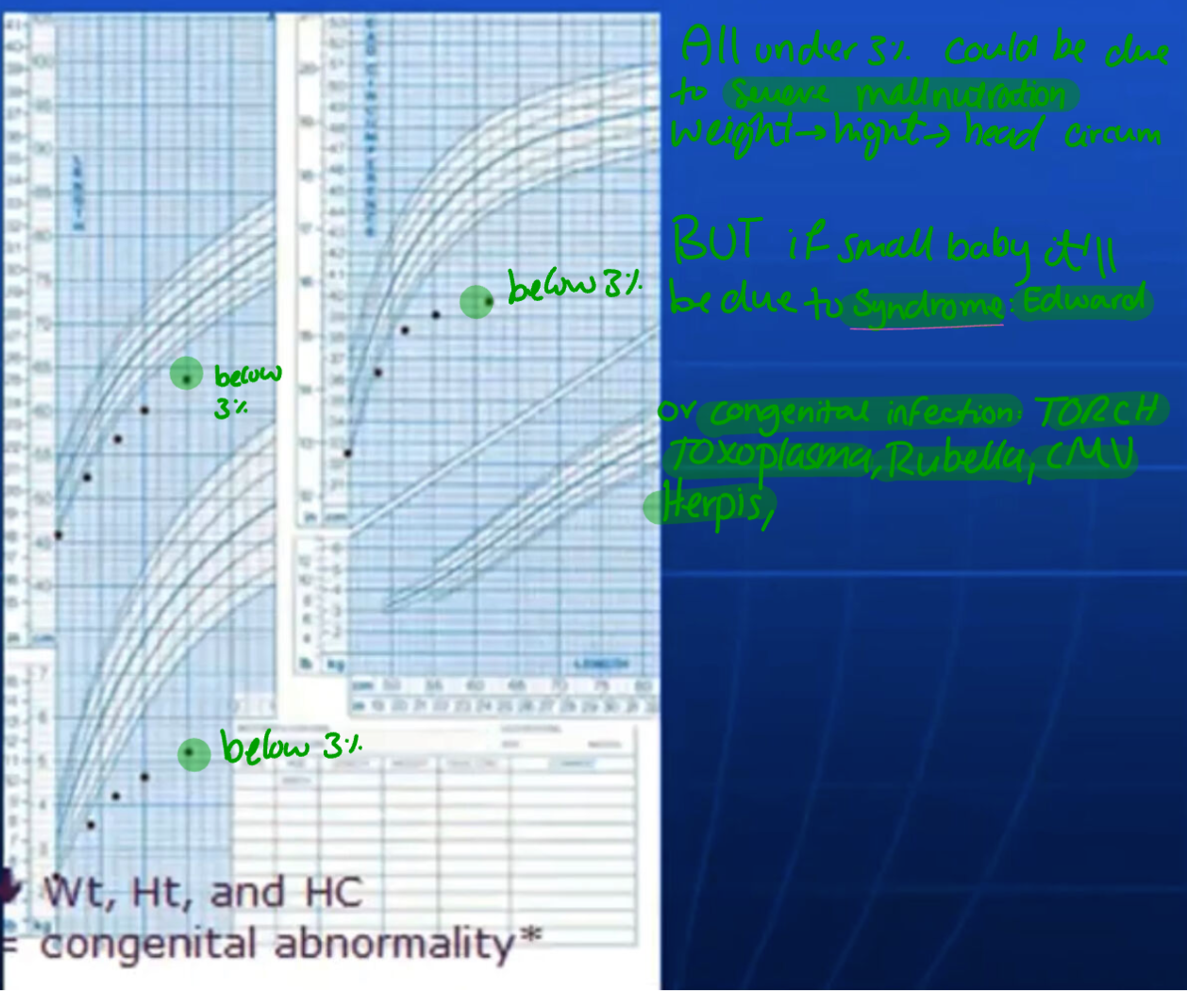
- Stunted Growth: Abnormal length and head circumference.
- Possible psychosocial dwarfism.
Causes of Failure to Thrive Y
All children with FTT are undernourished.
Methods to Categorize Undernutrition Y
| Degree of Undernutrition | GOMEZ: % Median Weight-for-Age | WATERLOW: % Median Weight-for-Height | McLaren READ: % Median Weight-to-Height |
|---|---|---|---|
| None | >90 | >90 | >90 |
| Mild | 75-90 | 80-90 | 85-90 |
| Moderate | 60-74 | 70-79 | 75-84 |
| Severe | <60 | <70 | <75 |
Clinical Subtypes Y
I. Medical Cause
- Organic vs. Non-organic vs. Mixed
II. Clinical Presentation
- Age of onset
- Severity
- Chronicity
Types of FTT Y
- Organic (30%): Secondary to a disease process; medical treatment needed.
- Non-organic (70%): Underfeeding and psychosocial disturbance; requires environmental change.
- Mixed: Combination of medical and environmental factors.
Systems Causing Failure to Thrive
Most Common to least common Y
- Gastrointestinal
- Neurological
- Respiratory-Pulmonary
- Cardiovascular
- Endocrine
- Others
Prevalence of Failure to Thrive Y
- 3.5% of admissions to children’s hospitals.
- 10% of clinic visits in urban and rural outpatient settings.
- Up to 16% of 0-4 year olds in low-income populations are “stunted.”
Diagnostic Evaluation Y
- Growth Assessment: Confirm diagnosis with current and past weight and height.
- History: Identify predisposing factors.
- Physical Examination: Look for significant findings other than malnutrition.
- Development-Behavioral Assessment: Assess delays in cognitive, language, or motor functioning and identify behavioral abnormalities.
- Laboratory Evaluation: Varies for each child; a stepwise approach is recommended.
- Directed by findings from history and physical examination.
- Document nutritional status: albumin, iron, zinc.
- Consider endemic problems: TB, AIDS, giardia.
- Nutritional and Feeding Evaluation: Assess content and structure of mealtimes and feeding techniques.
- Social History: Identify parental/family strengths and weaknesses.
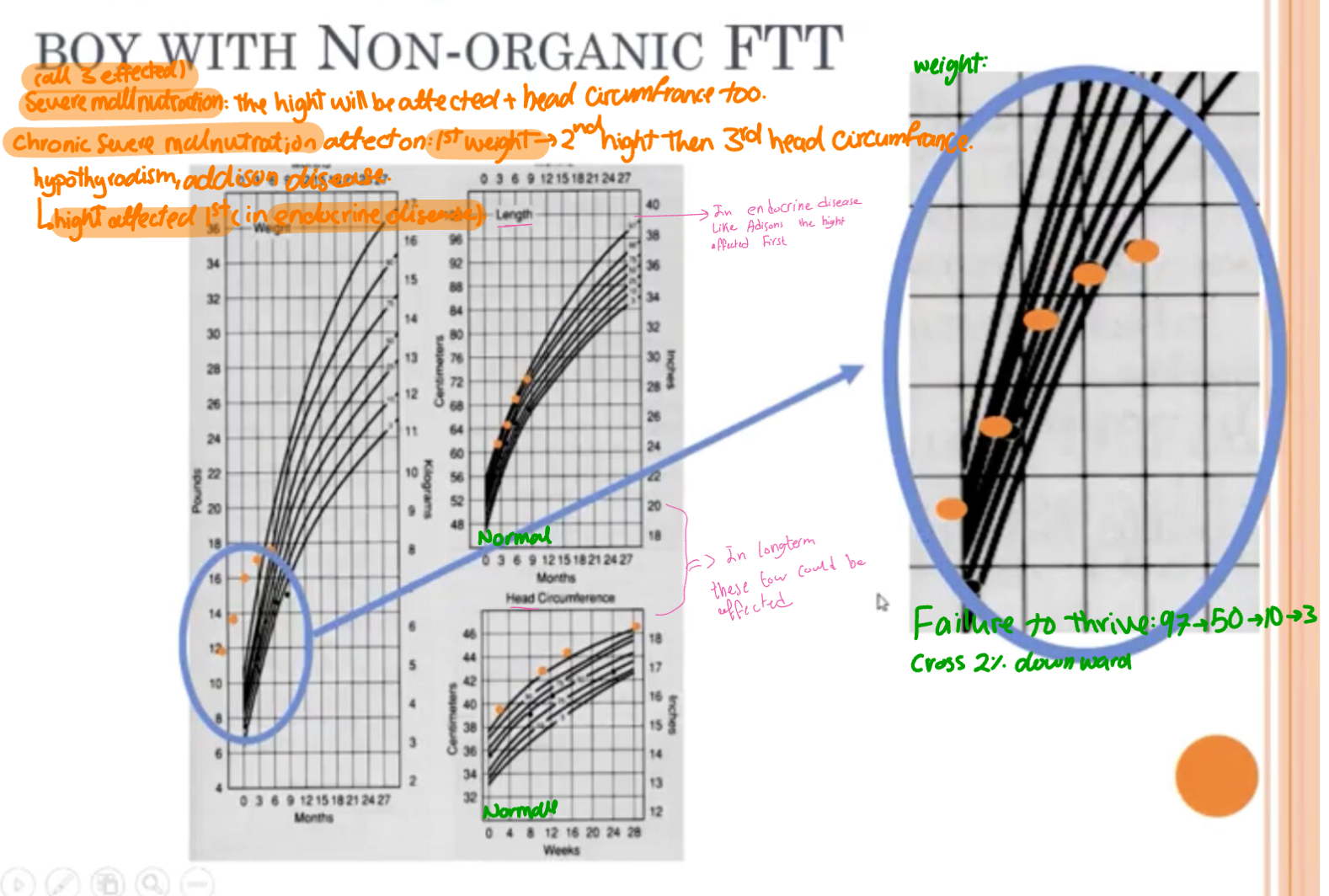
Case Study
Growth Charts of an 8-Month-Old Boy with Non-Organic FTT
-
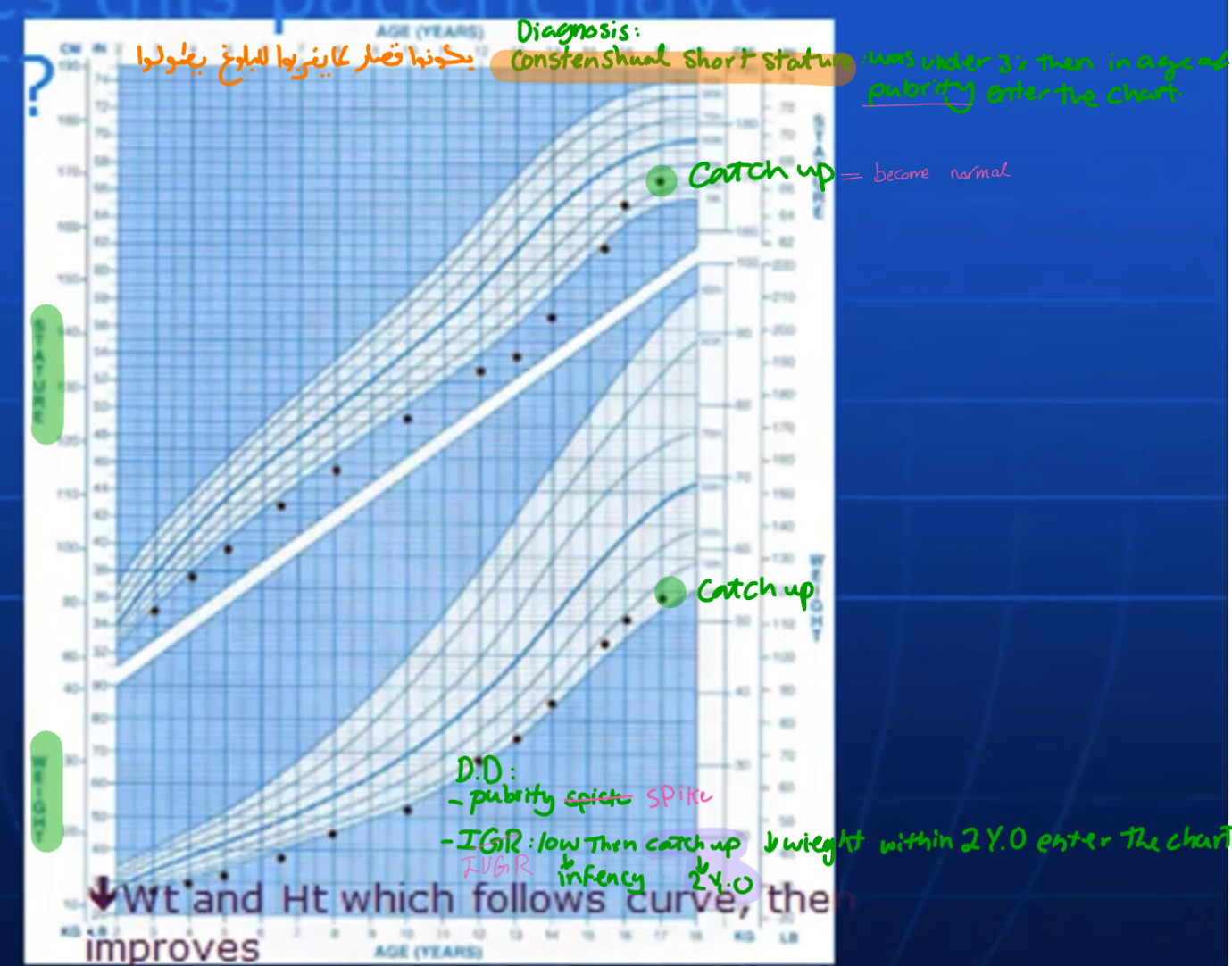
Stature-for-age and weight-for-age percentiles are used to track growth.
-
Weight and height should follow the curve to show improvement.
Conclusion
Failure to Thrive is a complex condition requiring a comprehensive approach to diagnosis and management, considering both medical and environmental factors.