Internal Medicine
Encephalitis
General Characteristics
Encephalitis is a diffuse inflammation of the brain parenchyma and is often seen simultaneously with meningitis. It is usually viral in origin. Nonviral causes, however, must also be considered.
The overall mortality associated with viral encephalitis is approximately 10%
Causes
-
Viral causes
- Herpes (HSV-1)
- Arbovirus: for example, Eastern equine encephalitis, West Nile virus (skin rashes)
- Enterovirus: for example, polio
- Less common causes (unvaccinated): for example, measles, mumps, EBV, CMV, VZV, and rabies; (Canines, bat)
-
Nonviral infectious causes
- Toxoplasmosis (Immunocompromised, reccurent abortion, hemeperesis; ring enhancing lesion, cat? - fundsocopy? --- ) CC
- Cerebral aspergillosis (Farmer)
- Trypanosoma gambiense and brucei causing African sleeping sickness, social withdrawl
-
Noninfectious causes:
- Metabolic encephalopathies: electrolyte disturbance, hepatic encephalopathy, and uremic encephalopathy.
- Drugs: gold compounds used for RA
- Prion diseases: Creutzfeldt-Jackob disease and Kuru (shifting protein)
- T-cell lymphoma
Risk Factors
- AIDS—patients with AIDS are especially at risk for toxoplasmosis when the CD4 count is <200 (pneumocytisis, cryptococ, br. lymphoma, oropharyngeal candiasis, )
- Other forms of immunosuppression like drug-induced
- Travel in underdeveloped countries
- Exposure to insect (e.g., mosquito) vector in endemic areas
- Exposure to certain wild animals (e.g., bats or dogs) in an endemic area for rabies
Clinical Features
Patients often have a prodrome of headache, malaise, and myalgias. Within hours to days, patients become more acutely ill.
Patients frequently have signs and symptoms of meningitis (e.g., headache, fever, photophobia, nuchal rigidity).
In addition, patients have altered sensorium, possibly including confusion, delirium, disorientation, and behavior abnormalities.
Focal neurologic findings (e.g., hemiparesis; Paraplegia, aphasia, cranial nerve lesions) and seizures may also be present.
myotrophic latelar sclerosis - ALS. motor neuron disease
Diagnosis
-
Routine laboratory tests (to rule out nonviral causes) include CXR (TB Aspergolossis, urine and blood cultures, urine toxicology screen, and serum chemistries.
-
Perform an LP to examine CSF, unless the patient has signs of significantly increased ICP. Lymphocytosis (>5 WBC/mL) with normal glucose is consistent with viral encephalitis (similar CSF as in viral meningitis). CSF cultures are usually negative.
-
CSF PCR is the most specific and sensitive test for diagnosing various viral encephalitis, including HSV-1, CMV, EBV, and VZV.
-
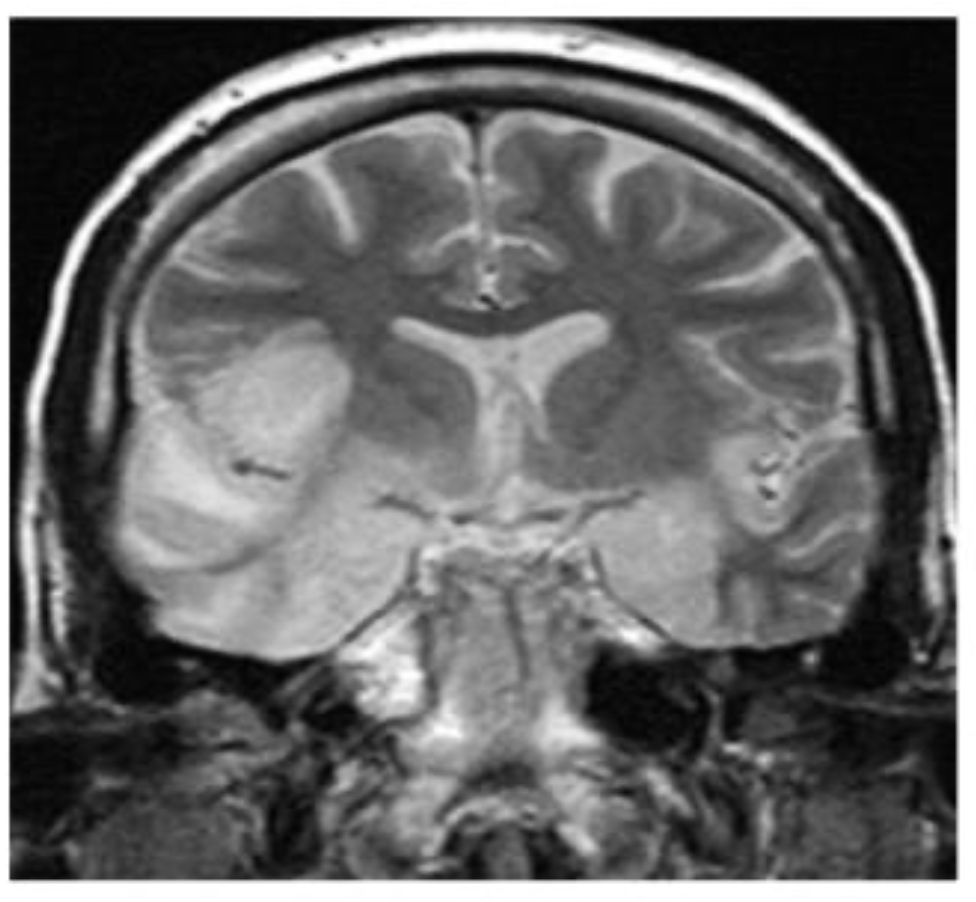
MRI of the brain is the imaging study of choice. Can rule out focal neurologic causes, such as an abscess.
- Increased areas of T2 signal in the frontotemporal (behind ear) localization are consistent with HSV encephalitis.
-
EEG can be helpful in diagnosing HSV-1 encephalitis, it would show unilateral or bilateral temporal lobe discharges.
-
Brain biopsy is indicated in an acutely ill patient with a focal, enhancing lesion on MRI without a clear diagnosis.
Lymphoma, toxoplasmosis are usually clear - otherwise brain biopsy
Treatment
-
Supportive care, mechanical ventilation if necessary
-
Antiviral therapy: There is no specific antiviral therapy for most causes of viral encephalitis.
- HSV encephalitis is treated by acyclovir for 2 to 3 weeks.
- CMV encephalitis is treated by ganciclovir or foscarnet (fundoscopy; Hemorrhage exudate;Pizza retina)
-
Management of possible complications:
Other notes
Loop;drug diagram + adverse CC spirinolactone
B1 Deficiency = Dry beriberi / Brain manifestation / eye manifestation- treat w/ thymine infusion
wet beriberi in heart; dilated cardiomyopathy
Pediatrics
Encephalitis is an acute inflammation of the brain.
Signs & Symptoms
- Headache, fever, confusion, drowsiness, and fatigue.
More Advanced Symptoms Include:
- Seizures, tremors, hallucinations, and memory problems.
- Younger children or infants may present irritability, poor appetite, and fever.
Causes
Viral
The most common causes of acute viral encephalitis are:
- Herpes simplex (most common cause)
- Varicella-zoster virus
- Poliovirus
- Measles virus
- Rabies virus
- John Cunningham virus
Bacterial
- Bacterial meningitis, spreading directly to the brain (primary encephalitis), or may be a complication of a current infectious disease like syphilis (secondary encephalitis).
Others
- Certain parasitic or protozoal infestations, such as toxoplasmosis, malaria, or primary amoebic meningoencephalitis (immunodeficiency).
- Fungal encephalitis like cryptococcus neoformans.
- Autoimmune encephalitis.
Diagnosis
-
Neurological examinations usually reveal a drowsy or confused patient. A stiff neck, due to the irritation of the meninges covering the brain, indicates that the patient has either meningitis or meningoencephalitis.
-
Examination of the cerebrospinal fluid obtained by a lumbar puncture procedure usually reveals increased amounts of protein and white blood cells with normal glucose.
-
CT scan often is not helpful.
-
Magnetic resonance imaging offers better resolution.
-
In patients with herpes simplex encephalitis, electroencephalograph (EEG) may show sharp waves in one or both of the temporal lobes.
-
Diagnosis is often made with detection of antibodies in the cerebrospinal fluid against a specific viral agent (such as herpes simplex virus) or by polymerase chain reaction.
Treatment
- Treatment is usually symptomatic. Reliably tested specific antiviral agents are few in number (e.g., acyclovir for herpes simplex virus).
- For Mycoplasma infection, parenteral tetracycline is given. Encephalitis due to Toxoplasma is treated by giving a combination of pyrimethamine and sulphadimidine.
- Corticosteroids (e.g., methylprednisolone) are used to reduce brain swelling and inflammation.