Notes Compiled by Abdullah Bohairi, Faisal Alkharji, Faris Alsomih
General Examination
Upper Limbs
-
Clubbing - Also indicates IBD, Cirrhosis
-
leukonychia; due to low albumin liver - (Stigmata of CLD) hepatosplenomegaly
-
Kolionychia (spooning); Iron deficiency anemia - GI Bleeding, Gastric Cancer, Gastrectomy
-
Palmar Erythema (Hypothenar Eminence) - Stigmata of CLD

-
Dupuytren’s contracture - Palmar tendon becomes thickened Stigmata of CLD - Alcohol

-
Hepatic tremor Flapping Tremor - indicating Hepatic encephalopathy;
-
Move your hands on forearm - look for AV fistula indicate renal failure (patient undergoes dialysis)
Face
-
Greet - check for Gingival Hyperplasia indicating Transplanted Kidney; due Immunosuppressants (cyclosporins) + Acute Myeloid Leukemia in children
-
In children, a bleeding tendency and splenomegaly can be symptoms of Acute Myeloid Leukemia (AML)
-
then go to the face look for Jaundice (Look Down) & Anemia (Look Up) - use your thumb, makes sure there is good light source if not mention so Unilateral Jaundice - Retinoblastoma - must be replaced for glass eye
-
Anterior uveitis and scleritis are eye conditions that typically present with pain.
-
Episcleritis is an eye condition that generally does not present with pain.
-
Crohn’s disease, an inflammatory bowel disease (IBD), can cause red eyes.
-
Wasting temporalis muscle due cachexia manifestation; indicating tumors and stigmata of CLD
-
Cushingoid features - possibly due to Crohn’s disease treatment or post-transplant medications
-
Parotid Enlargement - stigmata CLD - Alcohol
-
Hepatitis C due Needles; drug use, re use of needles
-
Hepatitis B due STDs; sex worker
-
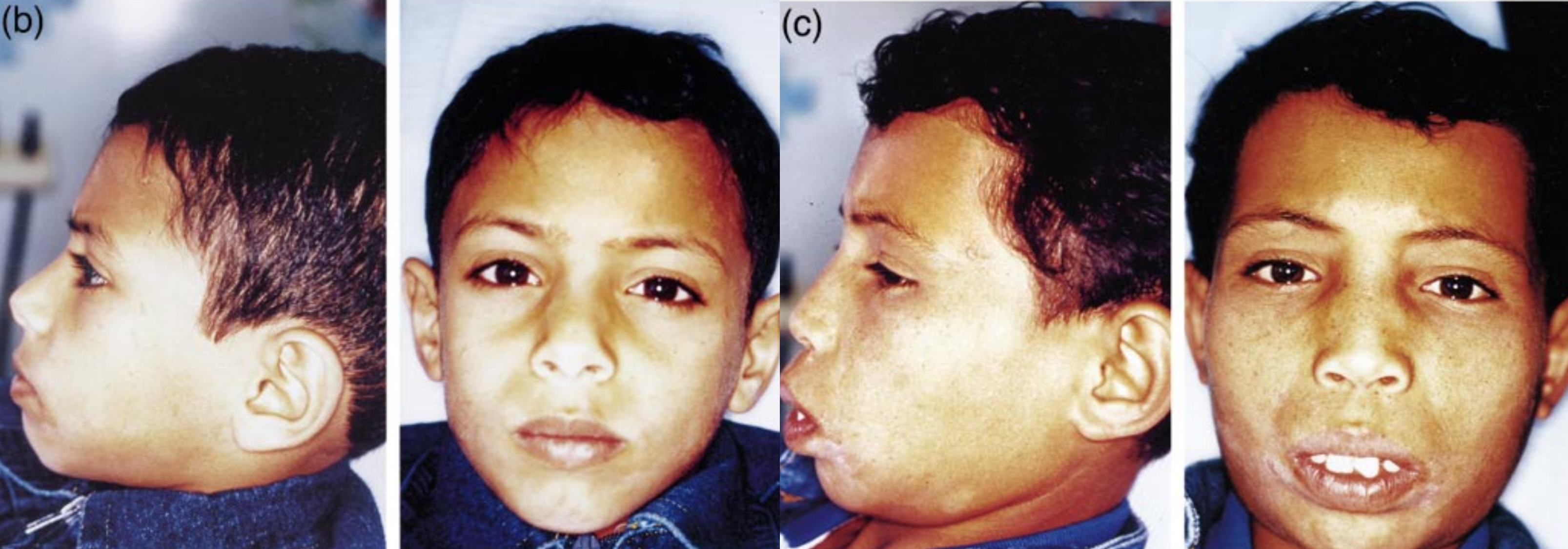
Thalasemia = Hepatomegaly + zygomatic bone prominence +
-
palmar erythema may indicate stigmata of CLD
-
Hemochromatosis or Recurrent blood transfusion; (± Infection hep. B & C) - results in increased iron can cause CLD CLD correlation with Normochromic normocytic (IBD;Crohns affect ileum b12 absorption) and microcytic hypochromic anemia (GI bleeding)
-
Pallor if CLD; portal hypertension; GI Bleeding; Varicosed veins + Dysfunction B12 due of Ileum malabsorption ± Crohns + Renal involvement
-
Angular Stomatitis (Geographic Tongue) - Malabsorption, B12 deficiency Ulcerative Colitis,
-
Aphthous ulcers; painful - due Crohns
-
Gingival Hyperplasia may result from following (Cyclosporin’s, CCB, Poor oral hygiene, Braces, Vitamin C deficiency)
-
Smooth Tongue - Iron Deficiency Anemia
-
Autoimmune hepatitis = CLD
-
Assess Thyroid Gland - association of other autoimmune diseases in liver
-
Phigner granumulatosis & aspergillosis cause unilateral eye exophthalmos along with saddle nose deformity - precipitating behind eye resulting in vasculitis
-
==For RESP eye goes out, sudden nose deformity = Unilateral Exophalamos due Granuloma behind the eyes ???? vasculitis??? - asperigilosis to perticipates to behind the eye (((Phigner granumulatosis & aspergelosis cause unilateral eye exophthalmos along with saddle nose deformity)))??== (check answer)
Chest
-
Spider naevus - press on it then remove your hand to check for any changes/reappearance is positive (stigmata CLD of chest) diagnostic +2
-
Gynecomastia (stigmata of CLD) - test for fluctuation with two fingers to assess firm tissues - may be using spironolactone which participates gynecomastia
-
Axilla hair distribution Acanthosis nigricans - indicating GI malignancy
Abdominal
-
Exposure flat, Until pubic symphysis - chest clear for stigmas
-
Abdomen Distended; Ascites, Umbilicus status
-
Scars; Liver transplant (mercedes benz scar).
-
if full of scars; (may not reached to diagnosis due to multiple scars)
- Crohn’s disease
- Familial Mediterranean Fever
- Porphyria; Enzyme Malfunction may lead to multiple skin scars
-
Caput Medusa (stigmata of CLD)
-
Cullen’s sign; Periumbilical + Grey Turner’s sign; Flank hemorrhages - (acute pancreatitis)
-
==Chronic liver = ++ Estrogen; Inverted hair distribution?== (check answer)
-
Scar of renal transplant is at the area of appendix
Lower Limb
- Pitting Edema (CLD) - warm your hand before palpation - press with two sides at same time for tibia, check patient eyes for any pain - comment findings
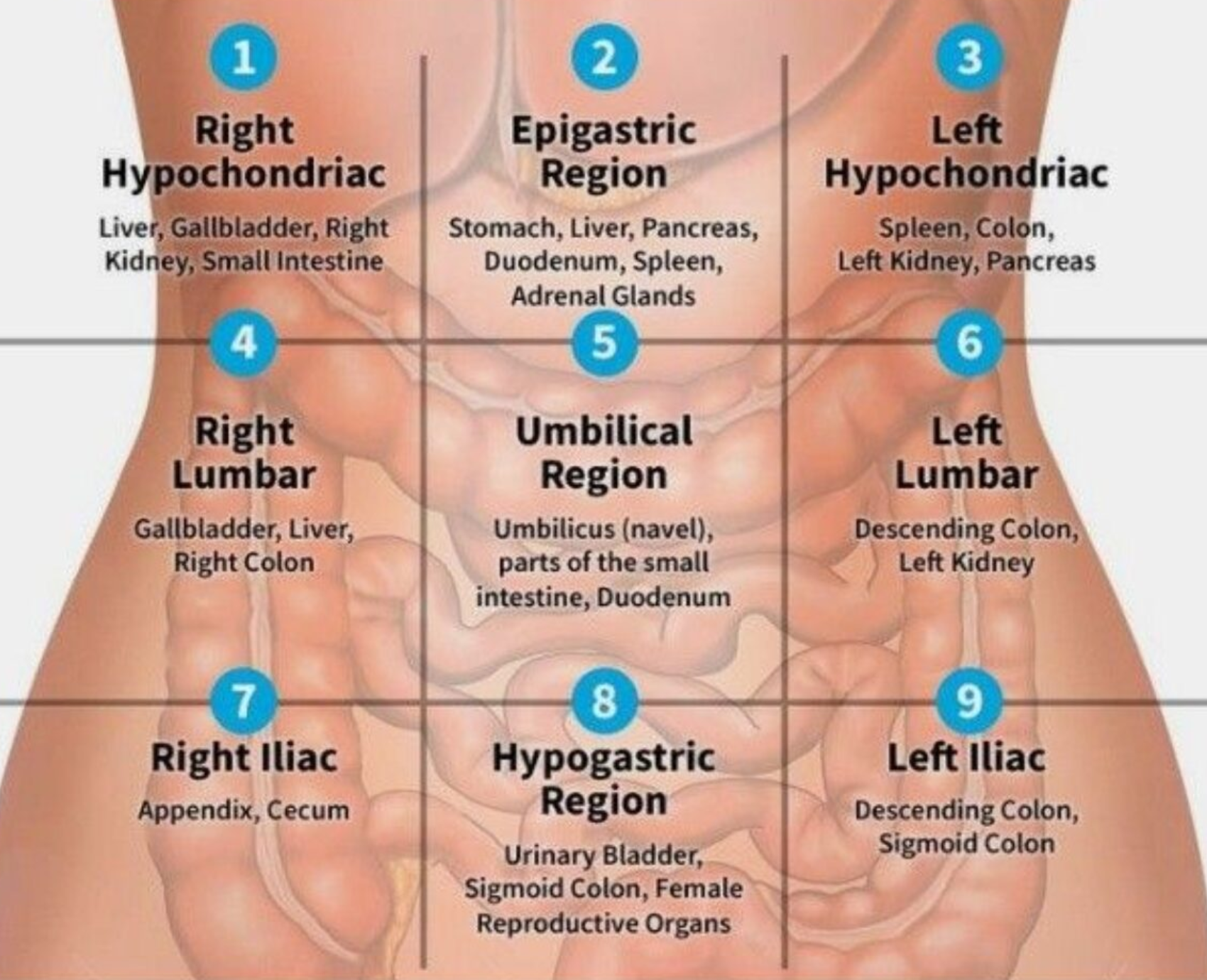
9 quadrants of abdomen
Superficial Palpation
Sit, Start from right iliac fossa with your eyes on the patient to check for any pain - ask patient if there’s any pain and avoid location if patient comment before hand (move in clockwise)
auscultation in the abdomen
-
venous hum (indicate portal hypertension) - soft systolic murmur - large volume of blood flows in umbilical and paraumbilical veins in falciparum ligament (portosystemic shunt)
-
hepatic bruit (indicating increase vasculature) - Heard over the liver, usually due to hepatocellular carcinoma, or vascular hepatic tumours
Liver Span
https://www.youtube.com/watch?v=DBif1jjAfKk
Palpation (lower margin by paplation wave way + upper margin by percussion)
- Keep your hand constant in movement, dont remove your hand for palpation position
- At ends of liver palpate deeping with your finger, like wave form when going inside open your hands to palpate liver margins
liver is palpable but the span is normal think about organ ptosis after massive wt loss
Percussion
- Percuss two times only, Extend your fingers fully, Tidal Percussion, Hit in between the interphalangeal joint
- With patient breathing out, test each costal margins
- when dullness appear let patient breath in, when its resonance it confirms location of liver
then comment on liver span Liver span is normally 6 to 12 cm in the midclavicular line
Causes of Tender Hepatomegaly
- Portal Hypertension; 1st answer
- Right sided Heart Failure
- Bud Chiari malformation (BCS) - pip on hepatic vein closed = congested
- Early Stage Cirrhosis
- Liver Fibrosis - Schistosoma mansoni ( or schistosomiasis hematuria)
- Schwannoma cell carcinoma - spleen, shifting dullness
- Infections - Malaria - visceral leishmaniasis (kalazar)
- Hodgkin’s lymphomas, Thalasemia, Leukemias
- Hepatomegaly; Hypoglycemia due - Glycogen Stomach disease - gusher disease
- Metastasis (with irregular surface)
- Primary liver tumor - alpha toxins
- Thalasemia
- malaria-visceral leishmaniasis
Causes of Hepatosplenomegaly
-
heptosplenomegally + stigamta of CLD = CLD even if you find one stigmata
-
hepatosplenomegally + jaundice + pallor = likely thalasemia/hemolytic anaemia
-
hepatosplenomegally + pallor = likely myloprolifertive disorder like leukemia
-
hepatosplenomegally + pallor lymphnodes =
- likely lymphoproliferative disorder like lymphoma or
- visceral leishmaniasis ( kalazar )
-
Hepatosplenomegally only + frequent attacks of hypoglycemia in young patient = most likely this glycogen storage disease like von geirk disease
-
hepatosplenomegally + short stature and mental retardation = lysosomal storage disease
Spleen
https://www.youtube.com/watch?v=rKsqO1tAKvs
- Deep breath for palpation
- waveform
- Dont Act - Relax your fingers
- Not palpable in healthy patient
Splenomegaly causes
-
splenomegaly only with skin rash induced by amoxicilin think about infectious mononucleosis
-
splenomegally only with Rhumatoid hand think about feltys syndrome
-
thalassemia + portal hypertension + malaria & Visceral leishmania
Kidney
https://www.youtube.com/watch?v=obIdJsgi_gs https://www.youtube.com/watch?v=Tr6CYu3GiKE
- Renal transplant Scar - located at Appendix right iliac fossa
Signs of renal failure;
- DM; finger presentation nail pitting, yellow brittle; more prone to fungal infections
Causes of palpable kidneys:
- Polycystic kidney disease
- Hydronephrosis
- Tumor; Renal cell carcinoma
- Wilms Tumor in children
- Amyloidosis infiltration
- HTN
How to differentiate kidney, spleen
-
Spleen has notch, enlarges Diagonally/Oblique, moves with respiration, not palpable, under rib cage cant go above it
-
Kidney enlarges Vertically, largely unrelated, Palpable , Ballottable, does not move with respiration
Ascites - Fluid thrill test
Severe ascites, will resulted in …
- main indicator by simple touch, with slight movement of abdominal region
- Put hand on other side, and stimulate the abdomen from opposite side - (((whilst asking patient put their hand in midline))); to prevent transmission of fluid through anterior abdominal wall
shifting dullness
https://www.youtube.com/watch?v=Eog7addNRwc
Mild to moderate ascites are usually on flanks - You can check by percussion -
-
(((place hands by midline))), dullness progressively getting more by flanks Light percussion middle midline for shifting dullness - Between 3rd and 1st space between umbilicus then percussion rest check for ressonance/Dullness
-
to assure its ascites or mass; keep hand same position by 20-30 seconds;
-
do the percussion again after shift other side, then after 10 seconds for viscera of fluids to descend - percuss to check… switching patient to other side; if mass it will be dull - if ascites the fluid directed downwards resulting in shifting dullness & resonance -
Causes of Ascites;
Ascites assessment: Fluid thrill and shifting dullness
Transudate; Protein is low in fluid
- Heart Failure; Hydrostatic Pressure
- Liver Failure; Cirrhosis; Fibrosis
- Renal Failure; Nephrotic Syndrome
- Protein loosing enteropathy
exudate: Increased protein
- Infection - Spontaneous bacterial peritonitis - SBP -
- Cancer of abdomen
- Meigs syndrome (benign ovarian tumor presents along with ascites and pleural effusion)
- Pseudoxanthoma peritonii - reticuli ??? (check answer)
- SBP + chemical peritonitis - pancreatitis
After finishing all examination mention and examine
- Lymph nodes,
- lower limbs,
- Per Rectal examination,
- Per vaginal if female
- Melenas,
- Temperature,
- Sacral Edema
Other notes
- Cut your nails prior to examination/exam
- Abdominal E
- 45 degrees if patient presents with ascites
- Patient with chronic liver disease case will be given in exam -
- uncold your hand prior to palpation
- Dont Wear Gloves, Wash your hands
- Dont percuss below umbilicus (Urinary Bladder)
- Dont wait validation from examiner - if he commented to do it again do so
- Dont raise your arm when going with continuem of percussion