Adults: Removal by direct laryngoscopy and if big, through laryngofissure.
Children: Repeated removal by direct laryngoscopy, microsurgery, and cryosurgery. No tracheostomy. Tracheostomy is closed after removal each time (larynx grows normal). No recurrence in adults, recurs rapidly till puberty in children. May turn malignant in adults, does not turn malignant in children.
In Adults
In Children
Single and true neoplasm.
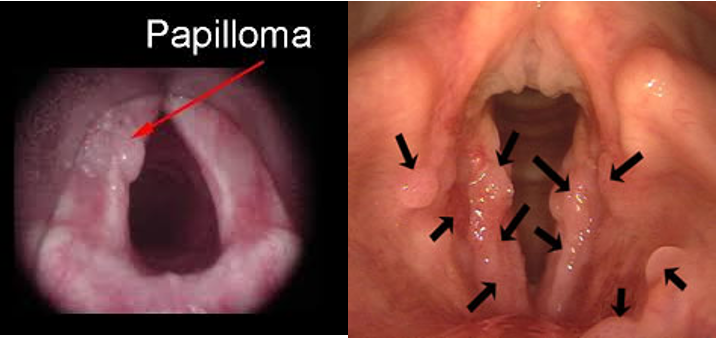
Multiple, viral or hormonal.
Causes hoarseness, rarely obstruction.
Causes stridor and hoarseness.
Exclusively cordal in anterior 1/2.
Multiple, affecting any part of the larynx.
Removal by direct laryngoscopy and if big, through laryngofissure.
Repeated removal by direct laryngoscopy, microsurgery, and cryosurgery.
No tracheostomy.
Tracheostomy, close it after removal each time (larynx grows normal).
No recurrence.
Recurs rapidly till puberty.
May turn malignant.
Does not turn malignant.
B. Malignant Tumors
Type: Usually squamous cell carcinoma.
Predisposing Factors: Leucoplakia, papilloma in adults.
Demographics: Over 40 years old, males more affected than females by 10:1.
Types
Glottic (on the cords) 70%
Supraglottic 20%
Subglottic 10%
Symptoms
Hoarseness appears early in cordal carcinoma, late in other types.
Dyspnoea and stridor early in subglottic carcinoma.
Discomfort in the throat early in supraglottic carcinoma.
Late pain due to invasion and perichondritis.
Dysphagia indicates infiltration of pharynx.
Haemoptysis, weight loss, and neck swelling as late symptoms.
Referred pain to the ear.
Signs
Laryngeal Examination:
Bilateral fungating mass in supraglottic tumors.
Unilateral thickening or roughness of vocal cords later on cauliflower mass in glottic tumor.
Bilateral ulcerofungating mass in subglottic tumor.
Fixation of vocal cords and tenderness of larynx due to perichondritis or its invasion.
Cervical Glands: Enlarged cervical glands and broadening of larynx.