IM
Minimal Change Disease (MCD)
Aetiology:
-
Children: Commonest NS; 75%
-
Adults: Hodgkin’s disease, chronic use of NSAIDs; Li, antibiotics.
-
Atopy: 30%
T-cell (immature CD34) and cytokine-mediated (IL-13) damage to glomerular BM → polyanion loss; resultant reduction of electrostatic charge → increased glomerular permeability to serum albumin.
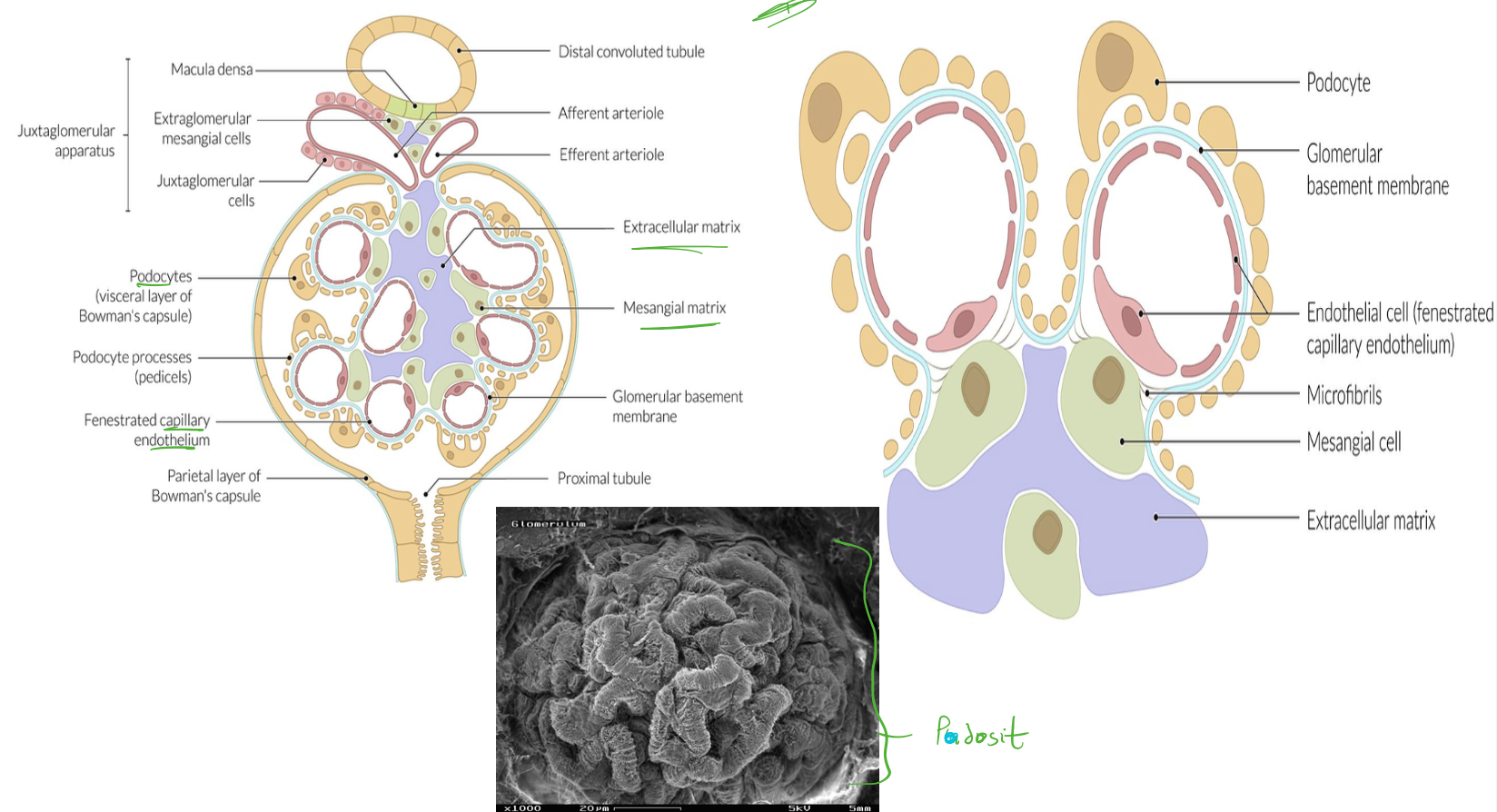
Pathology:
- Light microscopy is normal
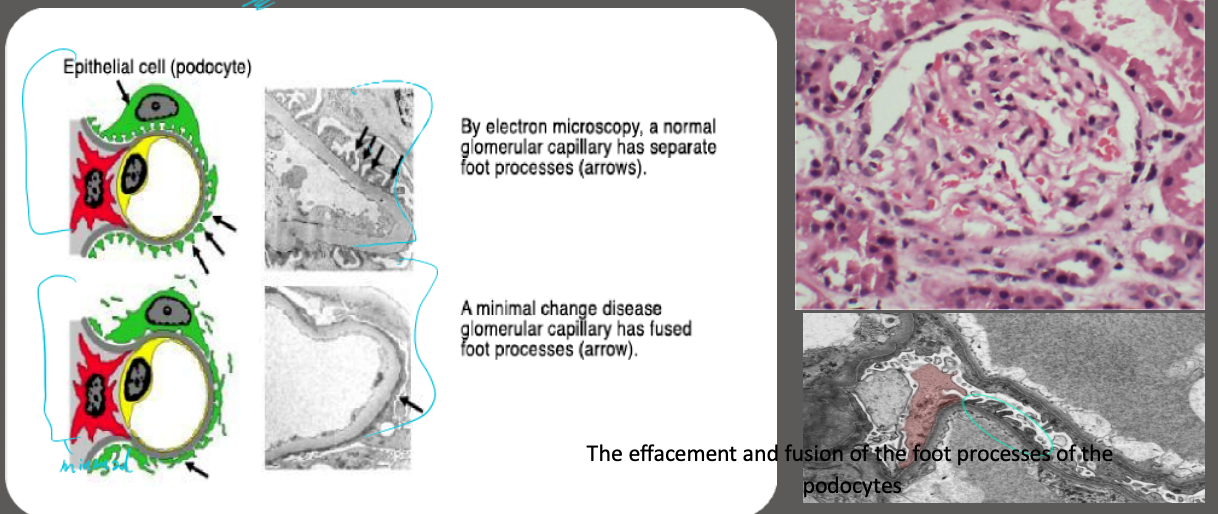
- EM: Fusion of podocyte foot processes
- IM: No immune deposits seen
- Selective glomerular proteinuria
Treatments:
- Steroids:
- Children: Highly responsive.
- Adults:
- Less response (repeat if relapse)
- Tapered Prednisone for 8-12 wks,
- Immunosuppressive therapy: Ciclosporin or tacrolimus, Rituximab Cyclophosphamide, levamisole
Excellent prognosis, No ESRD, Repeat if relapse
Image: The effacement and fusion of the foot processes of the podocytes
Case scenario:
A 14-year-old presented with swelling of both legs. Doppler ultrasound is negative for deep vein thrombosis (DVT) but shows diffuse subcutaneous oedema in both legs. Urinalysis reveals 3+ proteinuria and no other findings.
Blood results are as follows.
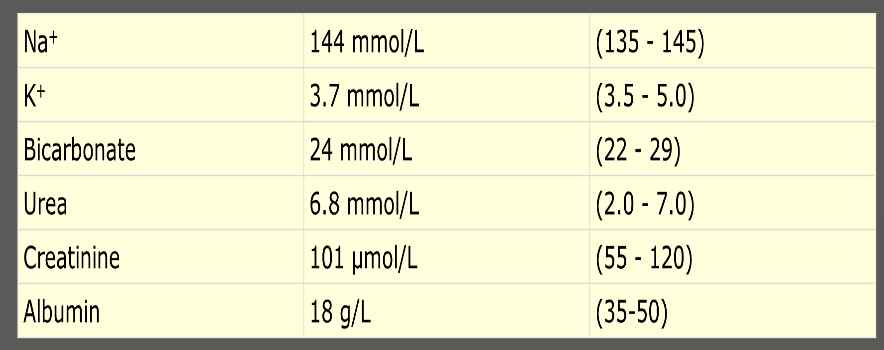
What initial course of action is appropriate here? A. Commence oral prednisolone B. Anticoagulate and repeat Doppler in one week C. Contact nephrologist to organise renal biopsy D. Organise plasma exchange E. Start IV cyclophosphamide
Pedia
Minimal Change Nephrotic Syndrome
- Age (yr): 2 - 6
- Sex (M:F): 2:1
- Nephrotic Syndrome: 100%
- Asymptomatic Proteinuria: 0
- Hematuria: 10 – 20%
- Hypertension: 10%
- Rate of Progression to Renal Failure: Non-progressive
- Associated Conditions: Usually none