Drug Eruption CS-OSPE






 This is a back of a 50 Y/O patient who is on oral antibiotics.
This is a back of a 50 Y/O patient who is on oral antibiotics.
Toxic Epidermal Necrolysis (TEN)
- Describe the skin condition? Generalized erythema, detachment of the skin
- What is the most likely diagnosis? Toxic epidermal necrolysis (because detachment of skin 30% or more)
- Pathology: Drug eruption, Acute skin failure.
-
What is the positive clinical sign confirms the diagnosis? Nikolsky sign
- More than 30% of skin is involved.
- Mucus membrane involvement - Conjunctiva
-
Differential Diagnosis:
- Steven Johnson syndrome - DRESS
- Pemphigus vulgaris - Bullous Pemphigoid
-
What is the management?
- Admission
- Antibiotic
- Correct the fluids, electrolyte, and protein
- Cover him for hypothermia
- Treat the underlying cause
-
Discuss the consequences of this condition if not treated appropriately? Infection, cardiac and renal failure, septicemia
- What area of the body you should check next?
Mucus membrane
- Oral
- Conjunctiva
- Genital



Stevens-Johnson Syndrome (SJS)
-
This child developed this manifestation after taking cephalosporin for chest infection, This is:
- SJS
- TEN
-
Pathology: Drug eruption, Acute skin failure.
-
Clinical Presentation:
- Involve 10% of the body surface.
- Involve the mucosal membrane.
-
Line of treatment:
- Admission to Burn Care unit**
- Nursing care.
- Monitoring hemodynamic changes.
- Fluid, electrolyte balance and nutrition.
- Prevention of complication (e.g. sepsis).
- identification of risk factors.
- Topical therapy.
- Admission to Burn Care unit**
- Lady came to ER and she was taking oral antibiotic; we noticed that there is redness in her body less than 3%. What is the diagnosis? SSSS / SJS
- What is the positive sign? Nikolsky sign.
Positive Nikolsky’s Sign
 Positive Nikolsky’s Sign
Nikolsky Sign : Dislodging of epidermis by lateral finger pressure in the vicinity of lesions, which leads to an erosion.
Shearing stresses on normal skin can cause new erosions to form
Positive Nikolsky’s Sign
Nikolsky Sign : Dislodging of epidermis by lateral finger pressure in the vicinity of lesions, which leads to an erosion.
Shearing stresses on normal skin can cause new erosions to form

Erythema Multiforme
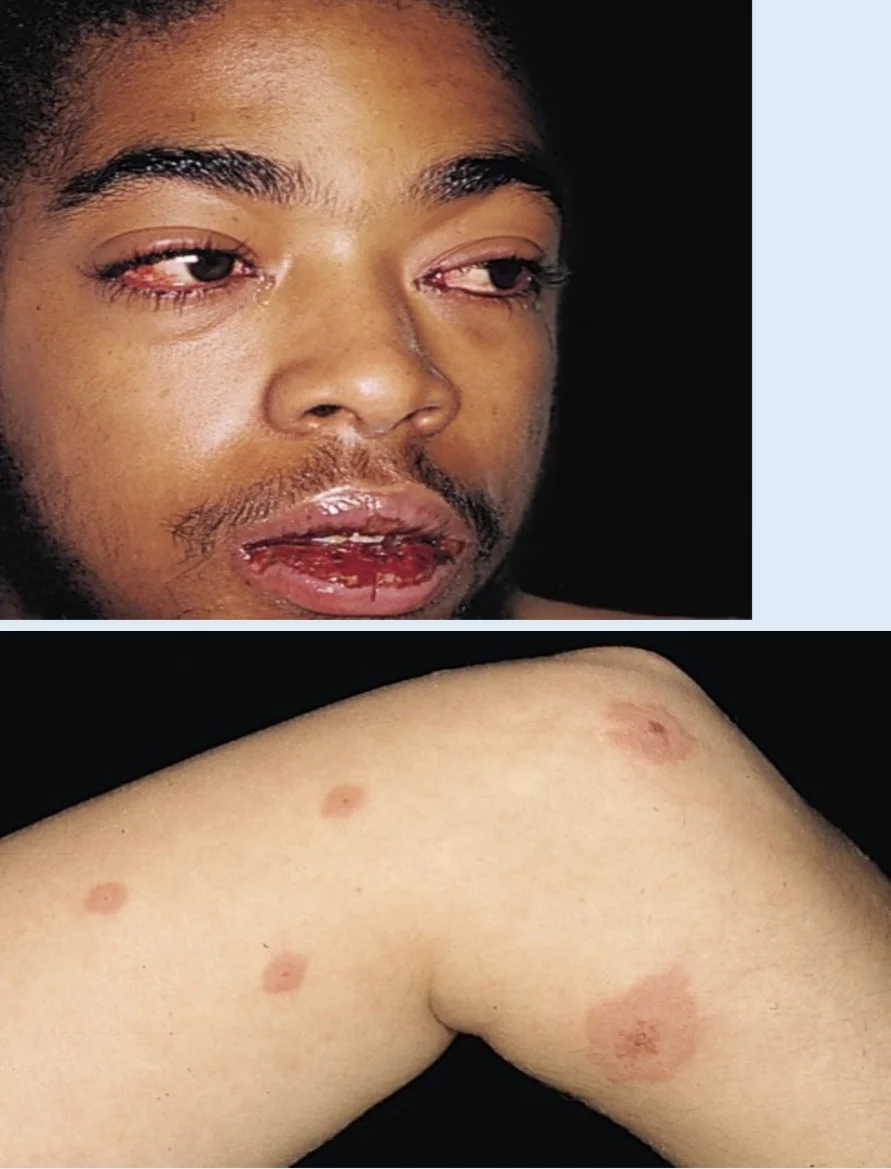
A 16 Y/O boy presents with a four-day history of oral erosions, eye pain, and cough. Exam reveals scattered targetoid plaques on the trunk (less than 3% body surface area) and superficial erosions on the lips and buccal mucosa with hemorrhagic crusting. widespread + oral Involvement
Girl with wheel appearance on her skin no more than 5h and oral involvement Dx?
- Erythema multiforme.
- What is the most likely diagnosis? Erythema multiforme
- Which is the characteristic skin finding of this disease? Target lesion
Treatment?
- Topical corticosteroid.


 This patient took cephalexin for the second time and had the same reaction at the same site.
This patient took cephalexin for the second time and had the same reaction at the same site.
Fixed Drug Eruption
What is the diagnosis?
- Fixed drug eruptions.
What is the clinical presentation?
- Begins as an erythematous, edematous plaque with a grayish center or frank bullae, then progresses to dark, post-inflammatory pigmentation.
What is the pathology?
- Drug eruption.
What is the treatment?
- Systemic + topical corticosteroids



Erythroderma
At midnight you have been called by the ER – resident to consult you about a 35 Y\O man who was brought in by his brother due to generalized redness of the body that almost involved all his body. His brother said that the condition started gradually last week and he got worse despite copious amounts of emollients he used in the last few days. His brother told you two weeks before he developed this condition, he received a short course of oral Prednisolone (steroid) prescribed by a chest physician due to chest allergy. When you examined him, he was shivering. With a lot of scales on his body and you noticed small, two thick, well-demarcated plaques on his elbows, he said they were here for six months. The vital signs are as follow: BP 115/65 mmHg, pulse 70 bpm, body temp 37.5c
-
Referring to the above scenario what is the emergency condition developed? Erythroderma
-
What is the diagnosis? Erythroderma
-
Mention three dermatological diseases may complicated by this condition? Psoriasis, chronic dermatitis, drug eruption, leukemia, lymphoma
-
What are the consequences of this condition? Hypothermia, high cardiac output failure, hypoalbuminemia, hyperkalemia
-
What is the management?
- Admission to Burn Care unit**
- Nursing care.
- Monitoring hemodynamic changes.
- Fluid, electrolyte balance and nutrition.
- Prevention of complication (e.g. sepsis).
- identification of risk factors.
- Topical therapy.
- Admission to Burn Care unit**

DRESS Syndrome Case
Case Scenario
A 34-year-old male known case of epilepsy for the past two years came to you suffering from high grade fever and some skin rash all over his body for the last 4 days. Patient mentioned that 2 weeks ago he had an episode of seizure so he took an anticonvulsant drug “phenobarbital”. On examination you find a papule and pustule in his trunk. Eosinophil was 2000mcl.
- What is your diagnosis? Dress syndrome - Pathology: Drug eruption.
- What is the cause from the scenario? *Ingestion of phenobarbital 2 weeks ago
- Clinical Presentation: rash and fever (87%), classically erythematous follicular papules and pustules, but may also include bullae or purpura.
- Mention 4 evidence from the history that support your diagnosis? Arrange it from the most imp. to least imp.
- How to manage your patient?

What is the diagnosis?
- Drug-induced exanthems.
What is the clinical presentation?
- Morbilliform, maculopapular eruptions.
What is the pathology?
- Hypersensitivity IV.
- Drug eruption.
What is the treatment?
- Antihistamines, topical steroids, and topical antipruritics.

What is the diagnosis?
- Hypersensitivity vasculitis.
What are the clinical presentations?
- Palpable purpura
- Maculopapular rash
What is the pathology?
- Drug eruption.
What is the treatment?
- Steroids.
- Immunosuppressants.
- Colchicine.
- Supportive care.
- Treatment of underlying conditions.