Insulin Hormone Structure
-
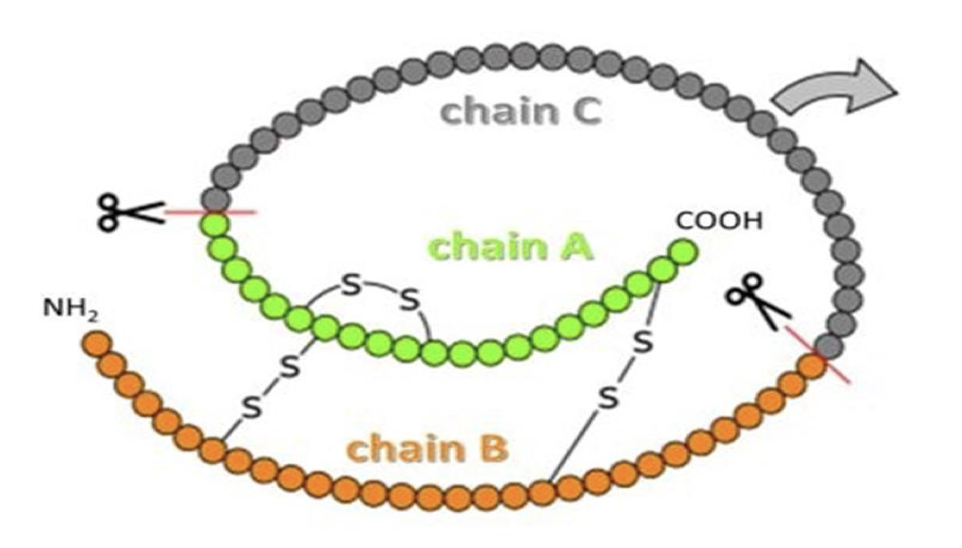
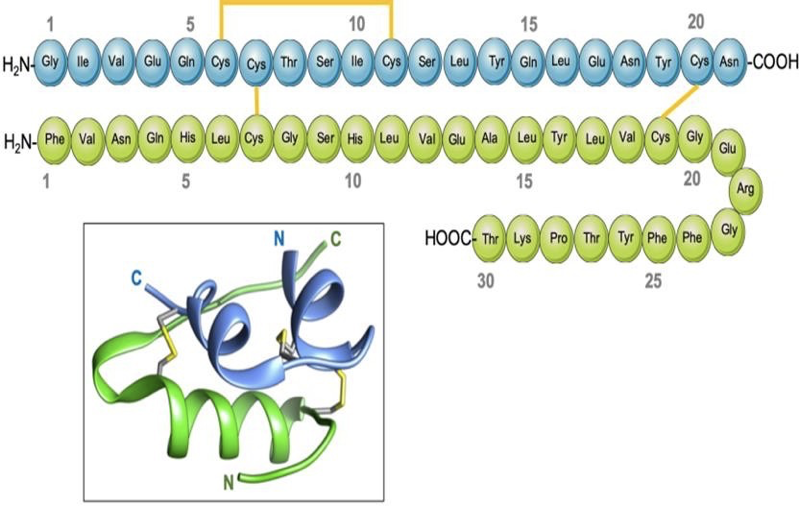
Insulin is a 51 amino acids protein hormone composed of two chains, A and B
-
Linked together by two disulfide bonds.
-
The A chain consists of 21 amino acids.
-
The B chain consists of 30 residues.
-
In the stored form, the two chains connected by C- peptide
-
Half-lives
-
The insulin and C-peptide are secreted in equimolar concentration.
-
Insulin has a short plasma half-life of 4-6 minutes.
-
This is because insulin needs to respond rapidly to changes in blood glucose.
-
The half-life of C-peptide is around 30 to 35 minutes.
-
The C-peptide used to measure the endogenous insulin secretion
Physiology of Insulin
Stored insulin
What is the importance of C-peptide level measurement?
Giving insulin level secretion
Insulin hormone
What is the importance of insulin level measurement?
Insulin Resistance measurement
Clinical disturbance due to insulin impairment
- Diabetes mellitus
- Insulin resistance
- Hyperinsulinemia
- Metabolic syndrome
Hormones that increase IR responsiveness and related diseases
- Growth hormone ⇒ Acromegaly
- Cortisol ⇒ Cushing Syndrome
- PRL ⇒ Hypogonadism
- Gonadal steroids ⇒ PCOS
Discussion
Why is insulin necessary physiologically? Why is insulin imbalance substantial clinically? insulin is dependent to satiety levels, any disturbance would cause constant hunger without substation (Polyphagia)
(Polyuria) Hyperglycemia, Hyperosmolarity, Glucose transporter 3 or 1 maximum
-
Treat underlying causes by reducing weight and increasing physical activity
-
Treat cardiovascular risk factors if they persist despite lifestyle modification
Keywords abstract
-
impaired glucose tolerance (IGT) “not diabetic”
-
NIDDM & Approx. 25% of nonobese individuals with normal glucose tolerance
-
Deterioration of glucose tolerance can only be prevented if beta-cell can increase its insulin secretory response and maintain a state of chronic hyperinsulinemea
-
Gross decompensation of glucose homeostasi occurs
-
Insulin supression of plasma insulin level, and glucose intolerence
-
Patients with NIDDM are also resistant to insulin supression of plasma FFA conentration.
-
FFA concentration elevations can be prevented if large amount of insulin can be secreted. - Free FFA results in Increased Hepatic Glucose production resulting in significant fasting hyperglycemia under these conditions
-
Hypertensive patients treated or untreated are insulin resistant, hyperglycemic, and hyperinsulinemic - a direct relationship between plasma insulin concentration and blood pressure has been noted.
-
Fructose-enriched diet in rats, lead to development of insnulin resistance and hyperinsulinemia.