Pemphigus Vulgaris (PV)
Pemphigus Vulgaris (PV)
- Pemphigus derived from the Greek pemphix meaning bubble or blister.
- Pemphigus describes a group of bullous diseases, originally named by Wichman in 1791.
Pathophysiology
-
Blisters in PV are associated with the binding of IgG autoantibodies to keratinocyte cell surface molecules.
-
The binding of autoantibodies results in a loss of cell-cell adhesion, a process termed acantholysis.
-
Pemphigus antibody binds to keratinocyte cell surface molecules desmoglein 1.
PV Characteristics
-
Histologically by intraepidermal blister
-
Histo-immunologically by the finding of IgGs bound keratinocytes desmosomes proteins.
-
Immunologically by circulating IgG autoantibodies in the serum of the patient directed against the cell surface of keratinocytes desmosomes proteins (desmoglein 1 ).
-
Clinically by flaccid bullae and or erosions in the mucus membranes and skin
Desmosomes ![[Pemphigus Vulgaris PV-1747635773679.webp|161x144]] ![[Pemphigus Vulgaris PV-1747635788142.webp]]
Clinical Presentation
Age
- Peak age of onset is from 50-60 years.
- The disease may present in childhood or in older persons.
- PV may be associated with other autoimmune diseases, particularly myasthenia gravis and thymoma.
Mucous Membranes
- Almost all patients have mucosal lesions.
- Mucosal lesions may precede the cutaneous lesions by 6 months.
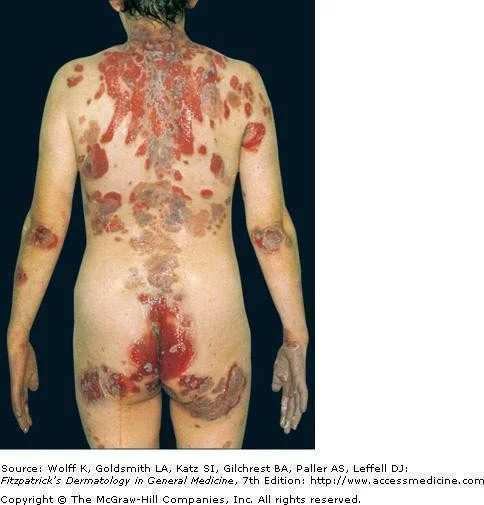
Skin
- Most patients develop cutaneous lesions.
- The primary lesion of PV is a flaccid bulla, which usually arises on normal-appearing skin.
- New bullae usually flaccid or become flaccid quickly.
- Affected skin often is painful but rarely pruritic.
- Nikolsky sign is positive.
- Asboe Hansen sign is positive.
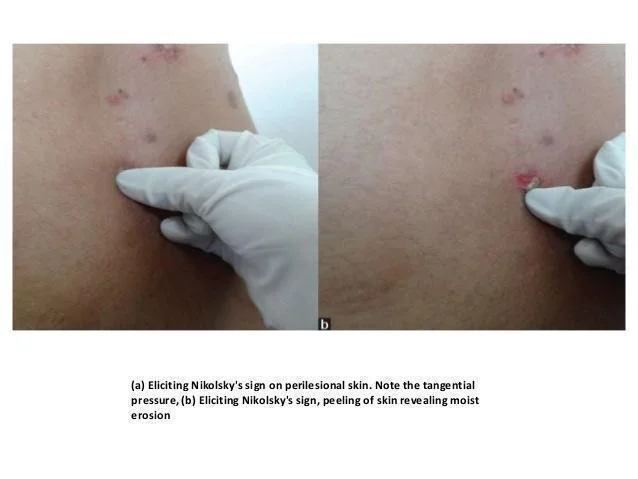
Positive Nikolsky’s Sign Nikolsky’s sign : Dislodging epidermis by lateral finger pressure in the vicinity of lesions, which leads to an erosion. Shearing stresses on normal skin can cause new erosions to form
- (a) Eliciting Nikolsky’s sign on perilesional skin. Note the tangential pressure.
- (b) Eliciting Nikolsky’s sign, peeling of skin revealing moist erosion


Differential Diagnosis
- Bullous Pemphigoid
- Dermatitis Herpetiformis
- Chronic bullous disease of childhood
Laboratory Studies
- To establish a diagnosis of PV, perform the following tests:
- Histopathology from the edge of a blister (Suprabasal epidermal separate from the basal cells to form clefts (the basal cells appear as tombstones)).
![[Pemphigus Vulgaris PV-1747636142118.webp]] ![[Pemphigus Vulgaris PV-1747636147538.webp]]
- Direct immunofluorescence (DIF) Note deposition of IgG around epidermal cells(net appearance ).
- Indirect immunofluorescence (IDIF) (Serum) using monkey esophagus: • Note binding of IgG antibodies to the epithelial cell surface. ![[Pemphigus Vulgaris PV-1747636158639.webp]]
Treatment
- The aim of treatment in PV is:
- Decrease blister formation
- Promote healing of blisters and erosions
- Determine the minimal dose of medication necessary to control the disease process and taking into account preexisting and coexisting conditions.
Drugs
-
Prednisone is 1-1.5 mg/kg/d
- Immunosuppressive drugs are steroid sparing and should be considered early in the course of the disease.
-
Azathioprine (Imuran)
- In conjunction with prednisone, the dose is 1 mg/kg/d
Prognosis
The severity and natural history of PV are variable, but before the advent of steroids, most patients with PV died.
Treatment with systemic steroids has reduced the mortality rate to 5-15%.