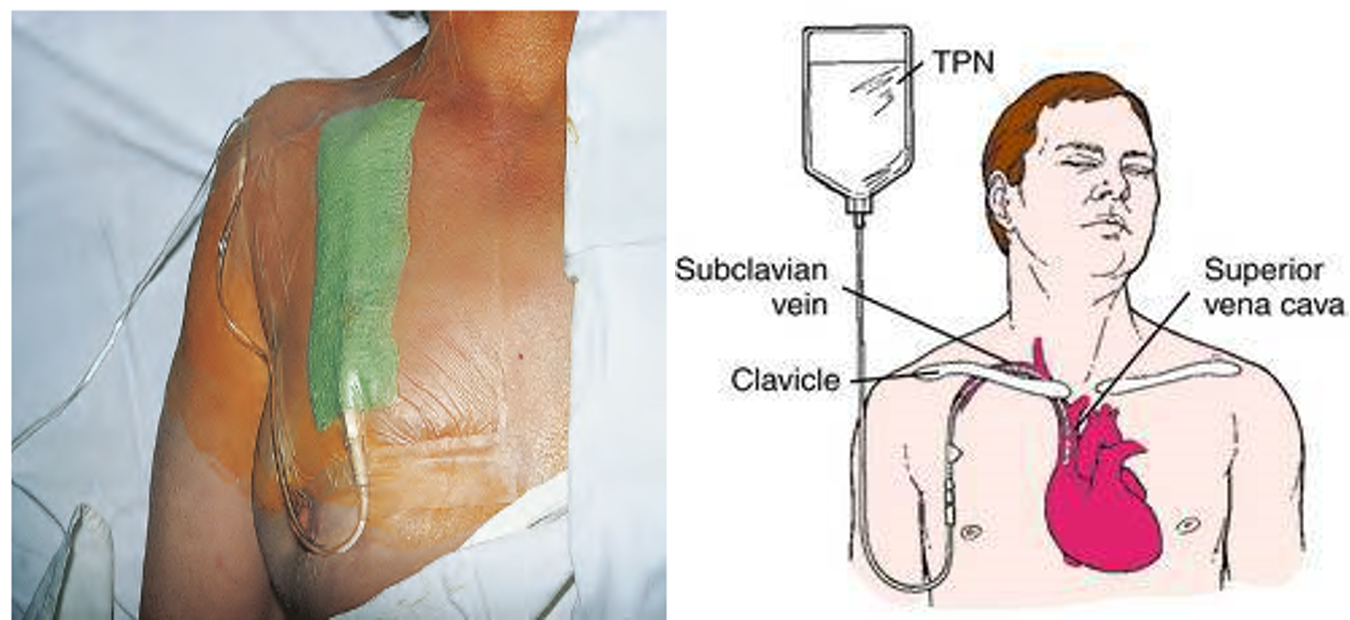
Total parenteral nutrition- TPN
Delivering predigested nutrients via hyperosmolar solution into venous system
-
TPN or CVN ( central venous nutrition ):
- Subclavian / Internal jugular,
- Catheter tip in SVC
- Most commonly used
-
PVN ( peripheral venous nutrition ) or PPN (partial parenteral nutrition):
- Solution of lower calorie, lower dextrose and higher lipid content
- Suitable for 7-10 days feeding
PPN (Peripheral Parenteral Nutrition) :
- TPN solutions have high osmolalities and can therefore, result in thrombophlebitis if given into a peripheral vein.
- In order to reduce the osmolality of PPN, the lipid content is increased as glucose-based solutions have high osmolality.
- Lipid is immunosuppressive.
TPN or CVN (Central venous route), when chosen, the catheter should be inserted via(access) either the subclavian, internal or external jugular vein and is tunneled subcutaneously to minimize the risk of infection.
-
Catheters used for delivering TPN should be single lumen catheters using an electronically controlled volumetric infusion pump.
-
TPN is usually given in an ‘all-in-one’ bag with a mixture of glucose, fat and l-amino acids combined with fluid, electrolytes, vitamins, minerals and trace elements
TPN - Indications
- Non-functioning GIT
- Short bowel syndrome
- Intestinal fistula
- Severe pancreatitis
- Intractable vomiting/ diarrhea
- Severe inflammatory bowel disease
- Developmental anomalies
- Multiple organ failure
- Severe malnutrition ( unable to take orally )
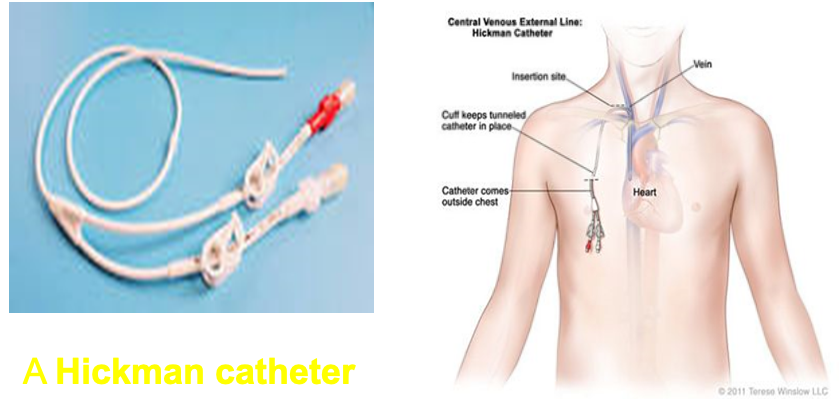
Home TPN
- Long term nutritional support
- Majority have malignancy
- Special catheter- e.g. Hickman
- Subclavian vein through subcutaneous tunnel
- Support system
Checks during Nutritional support
-
Daily – Full blood count (FBC), urea, electrolytes and blood sugar (Random).
-
Weekly – Liver function test, S.Albumin, trace elements.
-
Fortnightly – Vitamin B12, Zinc, Mn, Selenium, Copper, Iron, Transferrin.
Complications:
A. Related to feeding Catheter:
-
Catheter related sepsis –avoidance of catheter types that predispose to the development of infection, e.g. multiple lumen, non tunelled and femoral venous catheters.
-
Thrombotic complications include central venous and atrial thrombosis and thrombotic occlusion of the catheter.
-
Cardiac complications, e.g. perforation of the right atrium (when catheter is positioned in the Rt. atrium) and cardiac tamponade.
-
Thoracic duct injury.
-
Pneumothorax or hemothorax due to laceration of intrathoracic vein wall
Other TPN complications
- Electrolyte imbalances
- Acid-base imbalances
- Heart failure or pulmonary oedema
- Refeeding syndrome (in severely malnourished patients), which includes a rapid drop in potassium, magnesium, and phosphorus levels because of large flux of potassium and phosphate into the cells
To remember how to avoid the complication of refeeding syndrome when giving TPN to a severely malnourished patient, think “Start low and go slow.”