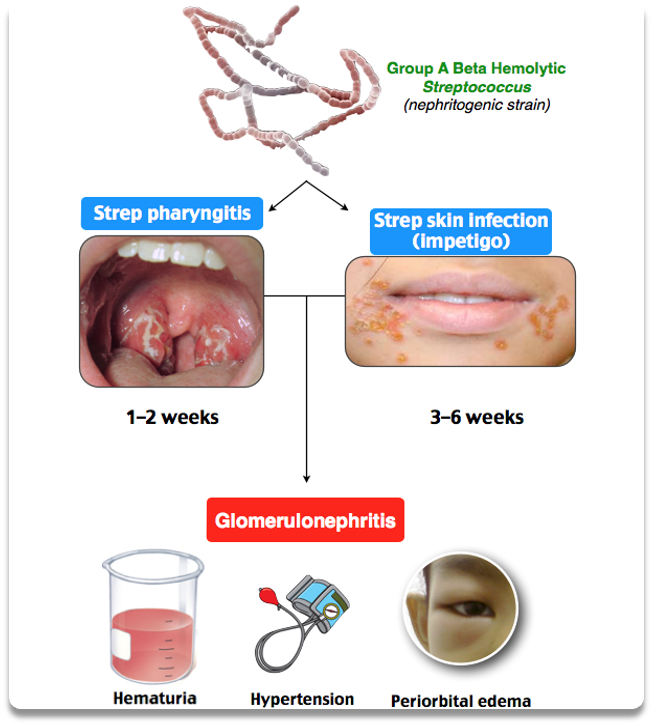
Acute Post-Streptococcal Glomerulonephritis
- Onset of reddish-brown (‘Coca Cola-colored’) urine 10–14 days after streptococcal throat or skin infection
- Deposition of immune complexes and complement in glomeruli
Clinical Presentation
- Most common in children between 5 and 15 years of age
- 1–2 weeks after streptococcal pharyngitis or 3–6 weeks after streptococcal pyoderma
- Nephritic presentation, various degrees of edema, HTN, and oliguria
- Encephalopathy and heart failure may develop
- Acute phase resolves in 6–8 weeks
- Proteinuria and HTN should normalize within 4–6 weeks after onset
- Microscopic hematuria may persist for up to 2 years, and the patient needs to be followed until its resolution
Investigations Include
- Throat swab
- Antistreptolysin O (ASO) titre; anti-DNAase B
- Typically ↓ C3, normal C4
- Biopsy if there is significant renal involvement – diffuse proliferative glomerulonephritis is seen, with crescents, in severe cases
Treatment
- Mainly supportive, with an excellent prognosis for recovery; in very severe cases involving renal failure, steroids have been used
- Note: Always check C3 and C4. Returns to normal 6-8 weeks after the onset. If still lowered, there may be another diagnosis, e.g., systemic lupus erythematosus or MCGN, which has much worse prognosis.