Enteral feeding
- Important in maintaining gut barrier function
- Intermittent bolus- suitable for stomach feeding
- Continuous - suitable for duodenum/ jejunum feeding
- Initiate at a slow rate, advance as tolerated
- Initially dilute feeds, gradually advance to full strength
- Feeding in semi-upright position (particularly for stomach feeds)
- Maintain this position for 2 hours after feeds
- Aspirate (stomach feeding) before next feed. >150ml- delay next feed.
Routes of enteral Nutrition
-
Oral — Patients who can eat normally.
-
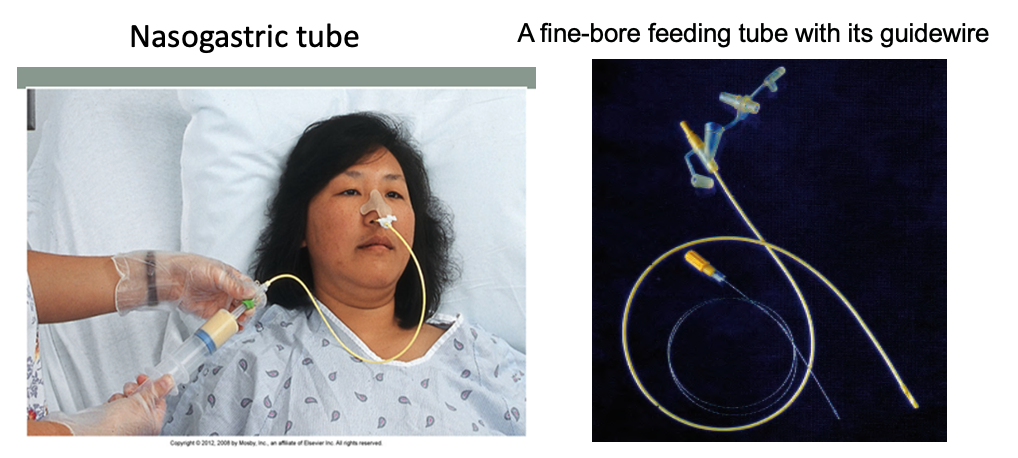
Nasogastric — Best for short-term nutritional supplementation.
-
Naso-enteric route is used if there is impaired gastric emptying or jejunal feeding is required, e.g pancreatitis.
- It can be established at laparotomy, endoscopically or radiologically.
- There are an increasing number of well-designed nasojejunal tubes for endoscopic placement, both single lumen and double lumen for simultaneous gastric drainage and Jejunal feeding.
-
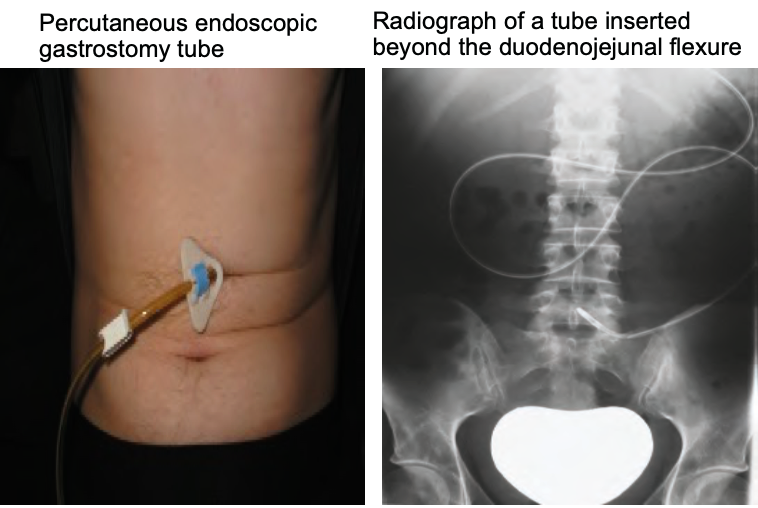
Percutaneous endoscopic gastrostomy (PEG) —It is achieved by incising over the illuminated tip of the endoscope while it is in the stomach and then “railroading a feeding tube” through the gastric and abdominal puncture hole. Indications: Mostly ‘neurological diseases’, e.g., stroke, motor neuron disease bulbar palsy & head injury etc.
Contraindication: — Complete esophageal obstruction.
Complications: are few (3%) but may be serious, e.g. sepsis or perforation of another viscus, e.g. colon.
-
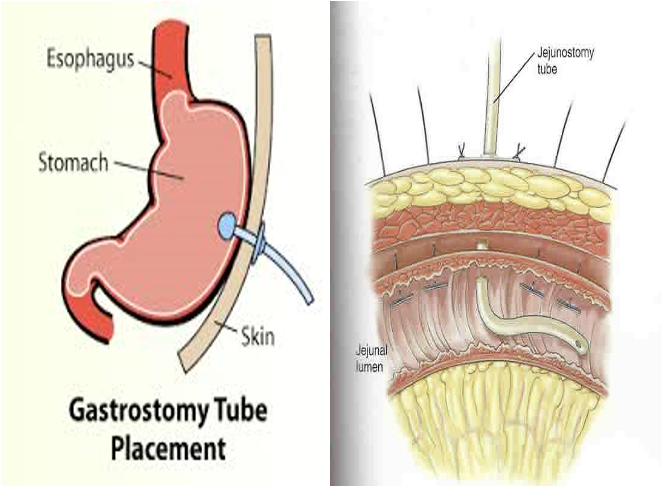
Feeding jejunostomy—Placement of the feeding tube is done at laparotomy when oral intake is not likely for seven or more days, e.g. - a- Major upper GI resections like esophagectomy, gastrectomy, pancreatoduodenectomy. - b- Major abdominal trauma or when having postoperative chemotherapy or radiotherapy.
Indications for enteral nutrition
- Malnutrition with functioning gut
- Post-operative feeding
Advantages of enteral feeding
- Simplicity
- Greater availability
- Lower cost
- Well tolerated
- Maintains gut integrity
- Fewer complications
Contraindications to enteral feeding
- Intestinal obstruction
- Paralytic ileus
- High output entero-cutaneous fistula
- Short bowel syndrome
- Severe acute pancreatitis
- Malabsorption
Complications of enteral feeding
- Mechanical: tracheobronchial intubation, erosion, blockage, displacement, bowel perforation
- Metabolic: Fluid/ electrolyte imbalance, hyperglycemia, Refeeding / overfeeding syndromes
- Gastrointestinal: Diarrhea, vomiting, pain
- Pulmonary: Aspiration
- Infection: Tube site