-
To assess breath sounds, ask the patient to breathe in and out slowly and deeply through the mouth.
-
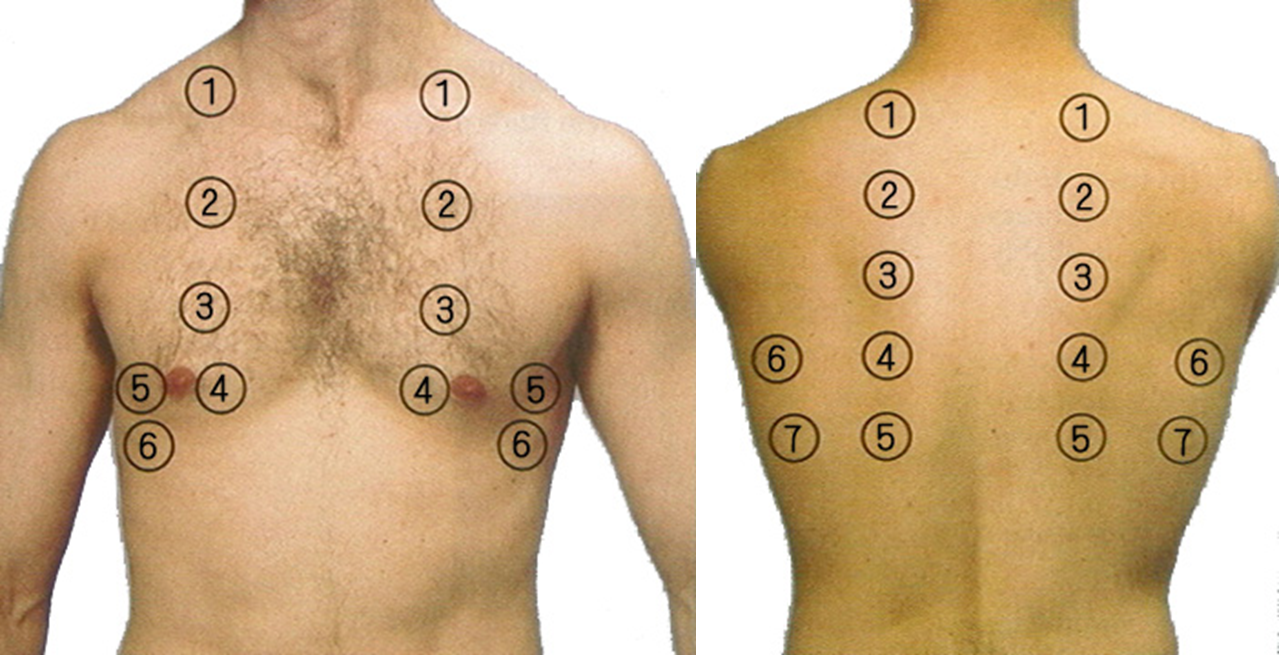
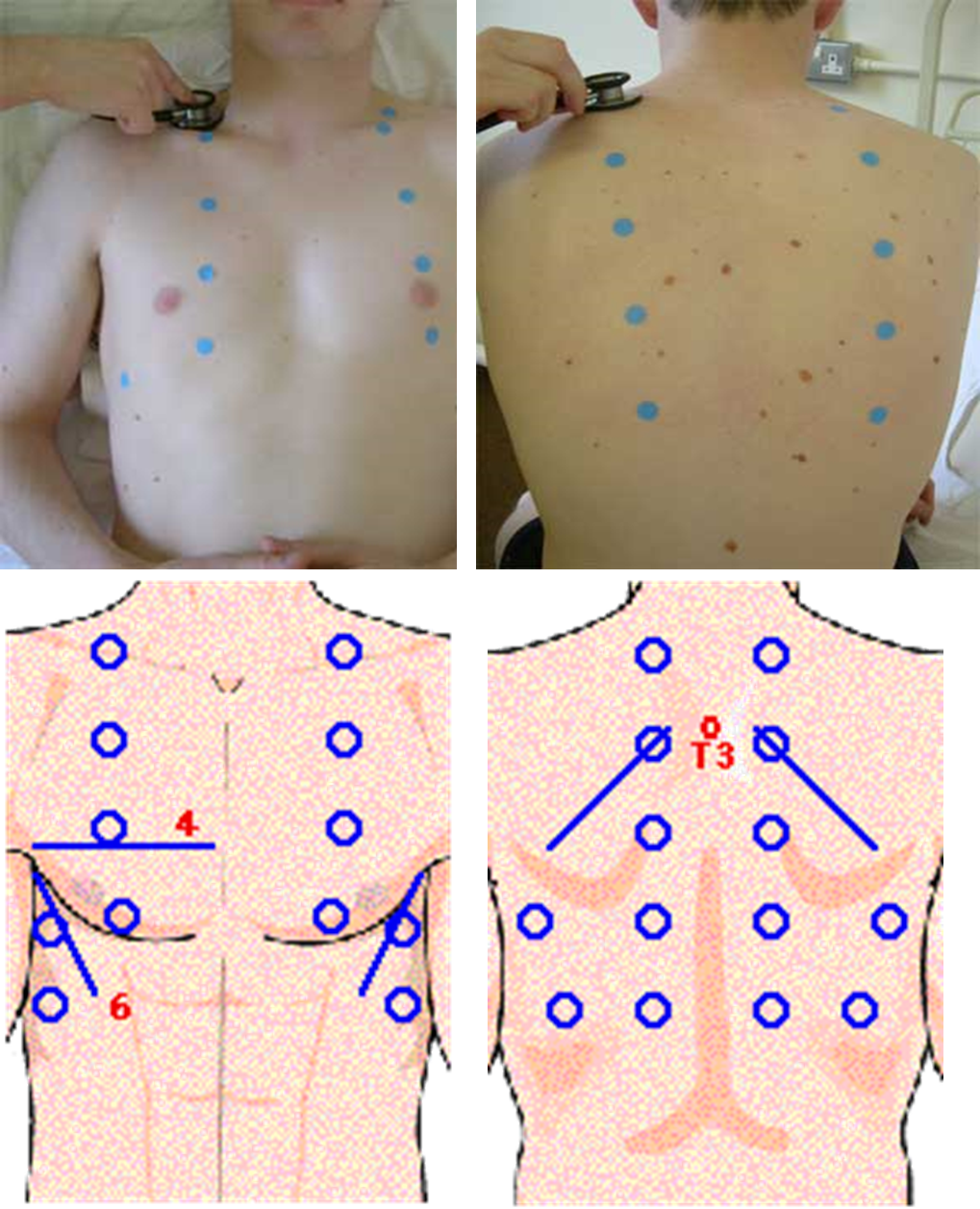
Begin at the apex of each lung and zigzag downward between intercostal spaces. Listen with the diaphragm portion of the stethoscope.
Process
- Using the diaphragm of a stethoscope & comment on the following:
- Breath sounds (BS)
- Intensity: Normal or ↓ as in (consolidation, collapse, pleural effusion, pneumothorax, lung fibrosis)
- Quality: Vesicular or bronchial
- Differentiation between vesicular & bronchial
- Vesicular: louder & longer on inspiration & has no gap between the 2 phases
- Bronchial: louder & longer on expiratory & has a gap between the 2 phases
Order of auscultation
Normal breath sound
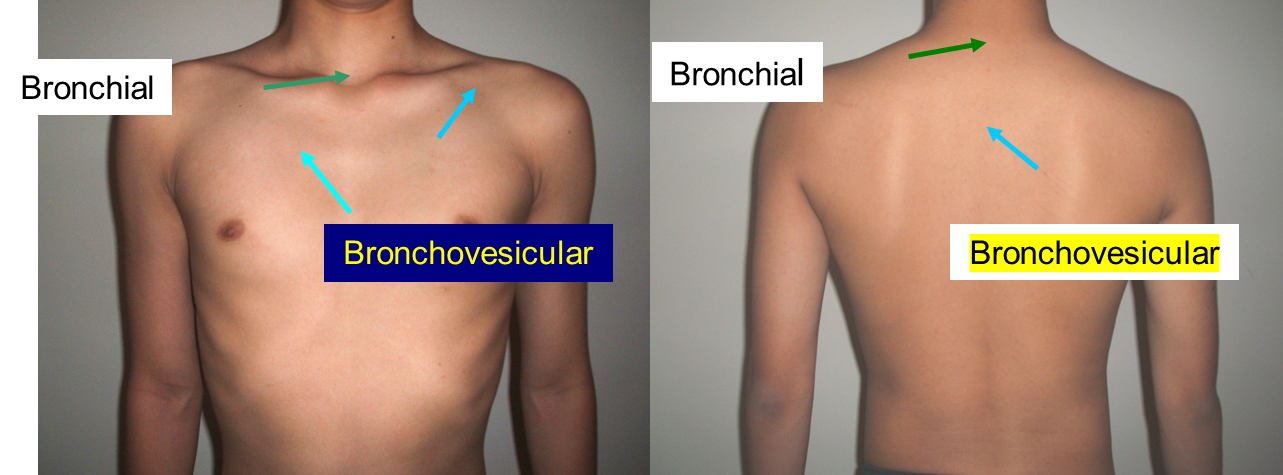
Tracheal breath sound
Bronchial breath sound
Larynx, suprasternal fossa, around 6th, 7th cervical vertebra, 1st, 2nd thoracic vertebra
Bronchovesicular breath sound
1st, 2nd intercostal space beside of sternum, the level of 3rd, 4th thoracic vertebra in interscaplar area, apex of lung
Vesicular breath sound
Most area of lungs
Lung sounds
- Bronchial
- Broncho-vesicular
- Vesicular
- Diminished
(cc) (COMB)
Other Notes
- Heart auscultation is mainly to detect heart abnormalities but severe lung disease may cause pulmonary hypertension and a loud P2
- Place the stethoscope over each of the five lobes of the lungs in turn, on the front and back of the chest. Ask the patient to take deep breaths in and out with their mouth open.
- Normal breath sounds are called vesicular. They are described as quiet and gentle. There is usually no gap between the inspiratory and expiratory phase sounds.
Bronchial breathing: - The sounds of bronchial breathing are generated by turbulent air flow in large airways (similar sounds can be heard in healthy patients by listening over the trachea. - Sounds are harsh and poor in nature. Unlike normal vesicular breath sounds, there is a gap between the inspiratory and expiratory phase sounds. - Bronchial breathing suggests consolidation or fibrosis, which permits the sound to be conducted more effectively to the chest wall.
Vocal resonance: Place the stethoscope at various levels over the back and ask the patient to whisper “ninety-nine” each time. Note how well the sound is transmitted The sound is muffled over a normal lung,
- increased if there is consolidation and decreased or
- absent if there is effusion or collapse
Whispering pectoriloquy: Is elicited as for vocal fremitus but ask the patient to whisper “one, two, three”. Whispering pectoriloquy is the increased quality and loudness of whispers that are heard with a stethoscope over an area of lung consolidation.