YEAST
- Candida albicans
- Pityrosporum: pityriasis versicolor & seborrheic dermatitis
Candida albicans
- It is a commensal flora of the gut which become pathogenic when the immune status of the person changed as in the following conditions:
- Physiological (old age, neonate and pregnancy)
- Pathological (DM, HIV and organ transplant)
- Long course of Antibiotics
Candida albicans
Mucosal Candidiasis
- Oral candidiasis i. Oral thrush ii. Angular cheilitis
- Genital candidiasis
Oral candidiasis
Oral candidiasis: thrush can be removed by rubbing with gauze

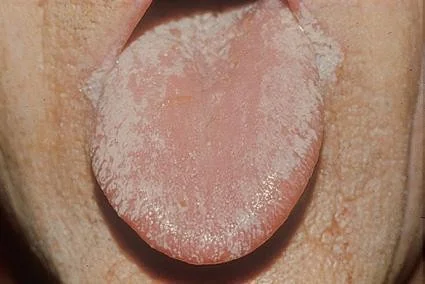
Candidiasis of the tongue
Angular cheilitis

Candida groin infection

satellite lesion seen in candiasis papule pastules at margins
Pityriasis versicolor
Pityrosporum orbiculare
- Asymptomatic
- Well demarcated brown patches over the trunk and upper extremities

 may appear specific time, with increased temperature or humidity or exercise
may appear specific time, with increased temperature or humidity or exercise
Mycetoma (Madura foot)
- Various species of fungus or actinomycetes may be involved.
- They gain access usually to the feet or legs, via a penetrating wound.
- The area becomes lumpy and distorted and developing multiple sinuses.
 discharge yellowish granule from sinuses
discharge yellowish granule from sinuses
Pus exuding from these sinuses shows tiny diagnostic granules. Treatment
- is Surgical and medical by systemic antibiotics or antifungal drugs, depending on the organism isolated.
Pityriasis rosea treatment
- Pityriasis rosea is self-limiting
- The mean duration is about 5 weeks
- More than 80% resolve by 8 weeks without treatment
- Most patients only need to be reassured
- About 25% request treatment for mild to severe pruritus
- Soothing anti-itch lotions available over-the-counter, topical steroids, and oral antihistamines may help
Case Two
Case Two: History
- HPI: Ali is a 17-year-old student . He presents for a routine college physical but mentions a scaly patch on his abdomen for the past few days. It itches a little bit.
- PMH: tonsillectomy as a child
- Allergies: penicillin (rash)
- Medications: none
- Family history: noncontributory
- Social history: college student; plays lacrosse; sexually active; moderate alcohol intake
- ROS: recent cold symptoms after moving into dorms
Skin Exam

- Ali ‘s exam shows a single erythematous oval plaque with scaling. What is the first test should you get during his office visit? a. Bacterial culture b. Gonorrhea culture c. Potassium hydroxide (KOH) exam d. Rapid plasma reagin e. Shave biopsy
Potassium hydroxide exam
-
Great job! You remembered that “All that scales must be scraped”
-
Rule out dermatophyte infections before moving forward on scaling rashes
-
In this case, the KOH exam is negative
-
This does not bother him much, so you give him a mid-potency topical steroid cream to use BID as needed for itching
-
Ali returns in 3 days for a rash on his chest, abdomen, and back
-
It only itches a little bit
-
Exam shows oval salmon-colored patches with minor scale; the oval patches follow skin tension lines on the back
-
Palms and soles are normal
-
Repeat KOH exam is negative

- Ali ‘s exam shows oval, salmon-colored scaling plaques on his trunk. What is the most likely diagnosis?
a. Guttate psoriasis (doesn’t follow skin tension lines) b. Nummular dermatitis (doesn’t follow skin tension lines) c. Pityriasis rosea d. Secondary syphilis (possible but not as common and does not have a herald patch) e. Tinea corporis (tinea incognito) (KOH negative)
Pityriasis rosea
-
Pityriasis rosea (PR) is an acute exanthematous eruption that mainly occurs in young people
- Most patients are between the ages of 10 and 35
- The peak incidence is in late teens and early 20s
- Some studies suggest a possible viral etiology, but this has not been definitively proven
-
Usually asymptomatic, but patients may have associated flu-like symptoms
- Malaise, nausea, loss of appetite, gastrointestinal upset, upper respiratory symptoms
- Less commonly fever, swollen lymph nodes, pain, or sore throat are noted
-
Classically starts with a “herald patch”
- Annular erythematous 2-10 cm patch anywhere on the body, with peripheral scaling and central clearing
- Patients often don’t remember or never had a herald patch
-
The secondary phase erupts in a “Christmas tree” pattern
- Similar oval patches and plaques erupt symmetrically over trunk and proximal extremities
- They follow relaxed skin tension lines, thus giving the appearance of a “Christmas tree” on the back
Now let’s look at a few examples of pityriasis rosea
The elusive “herald patch”





Pityriasis versicolor
Pityriasis versicolor is a common fungal infection that causes small, discolored patches on the skin.
Treatment options include topical antifungal medications, such as creams, lotions, or shampoos. In some cases, oral antifungal medications may be prescribed.

Pityriasis versicolor
Case One
Case One: History
- HPI: Mr. L is a 56-year-old man with several years of redness and scaling on his forehead, eyebrows, and central face. He does not complain of itching but is embarrassed by his appearance. It has not gotten better with moisturizers. It does not worsen with heat, exercise, hot foods or drinks, or alcohol.
- PMH: no major illnesses or hospitalizations
- Allergies: none
- Medications: ibuprofen as needed for headaches
- Family history: noncontributory
- Social history: office manager
- ROS: negative
Case One: Skin Exam

Case One, Question 1
- How would you describe the rash on Mr. L’s face? a. Erythematous macules b. Papules and pustules c. Thin scaling plaques d. Vesicles and crust
Case One, Question 2
- What is the most likely diagnosis for Mr. L? a. Actinic keratoses (scale in AK is keratotic, not greasy) b. Allergic contact dermatitis (he does not itch) c. Atopic dermatitis (wrong age; no history) d. Rosacea (no history) e. Seborrheic dermatitis
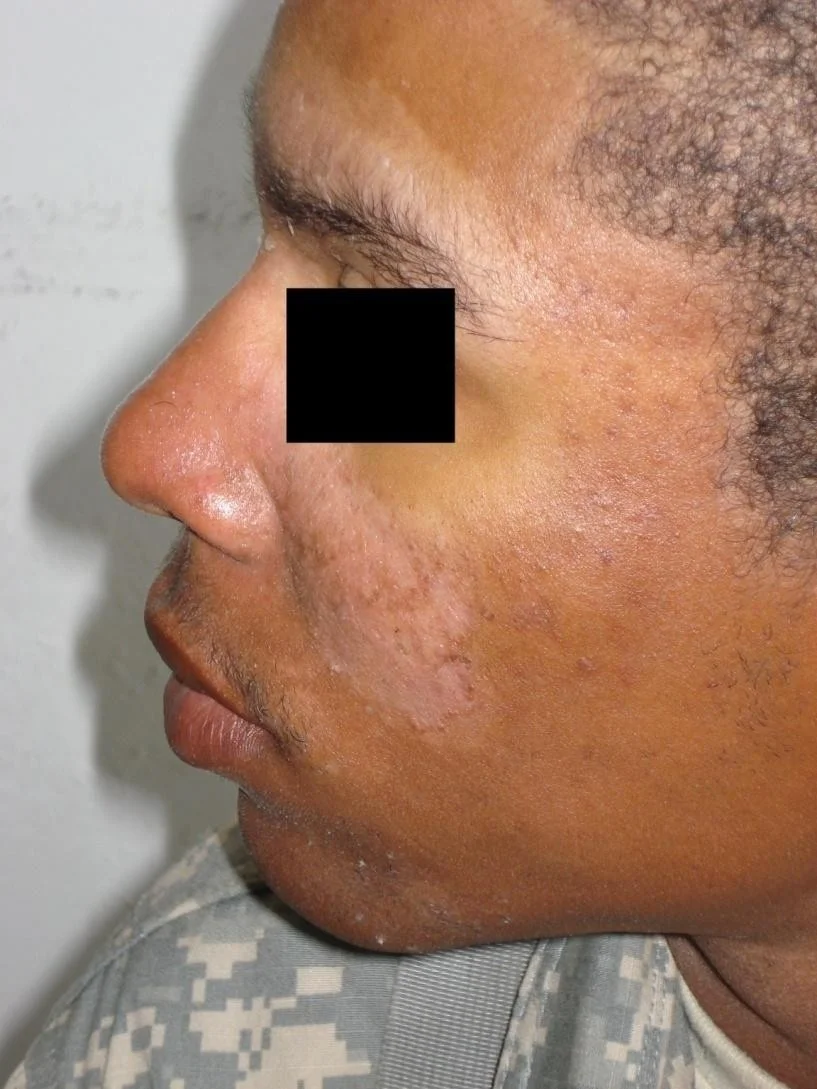
Seborrheic dermatitis
- Seborrheic dermatitis is a very common inflammatory reaction to the Malassezia furfur (Pityrosporum ovale) yeast that thrives on seborrheic (oil-producing) skin
- It presents as erythematous scaling patches on the scalp, hairline, eyebrows, eyelids, central face and nasolabial folds, external auditory canals, or central chest
- It can be hypopigmented, especially in darker skin types
- On the chest, it appears more central over the sternum
- Seborrheic dermatitis is often worse in patients with HIV
Here are some examples of seborrheic dermatitis
Seborrheic dermatitis


Seborrheic dermatitis


Seborrheic dermatitis


Seborrheic dermatitis
Often hypopigmented in darker skin types

Seborrheic dermatitis
Favors central chest
May be hypopigmented or erythematous


Case One, Question 3
- Which two of the following would be an appropriate treatment for Mr. L? a. Clobetasol proprionate cream (too potent) b. Desonide cream c. Erythromycin ointment (this is not bacterial) d. Ketoconazole cream e. 5-fluorouracil cream (for actinic keratoses)
Seborrheic dermatitis treatment
- Low-potency topical steroids (e.g. desonide) are safe to use for flares on the face
- Use twice daily for 1-2 weeks for flares
- Can also use topical ketoconazole or ciclopirox, or topical pimecrolimus, in the same manner
- Antidandruff shampoo for the scalp, chest
- Ketoconazole (Nizoral), selenium sulfide, zinc pyrithione shampoos
- Foam, leave on 10 minutes, rinse; repeat 3-5x/week
- Refer patients who fail these therapies