Liver injury
-
Susceptible to injury due to large size(1200-1600 g)
-
Covered by bony thoracic cage
-
Injury frequency - only 2nd after spleen( personal series)
-
Highly vascular- only 4% of body weight but 28% of total body blood flow
-
Double blood supply- portal vein & hepatic artery
-
Draining hepatic veins- short and thin walled
-
Spontaneous hemostasis- 50% of small lacerations
-
Profuse bleeding is from deep hepatic lacerations
-
Mortality: 8%- 10% Morbidity: 18%-30%.
-
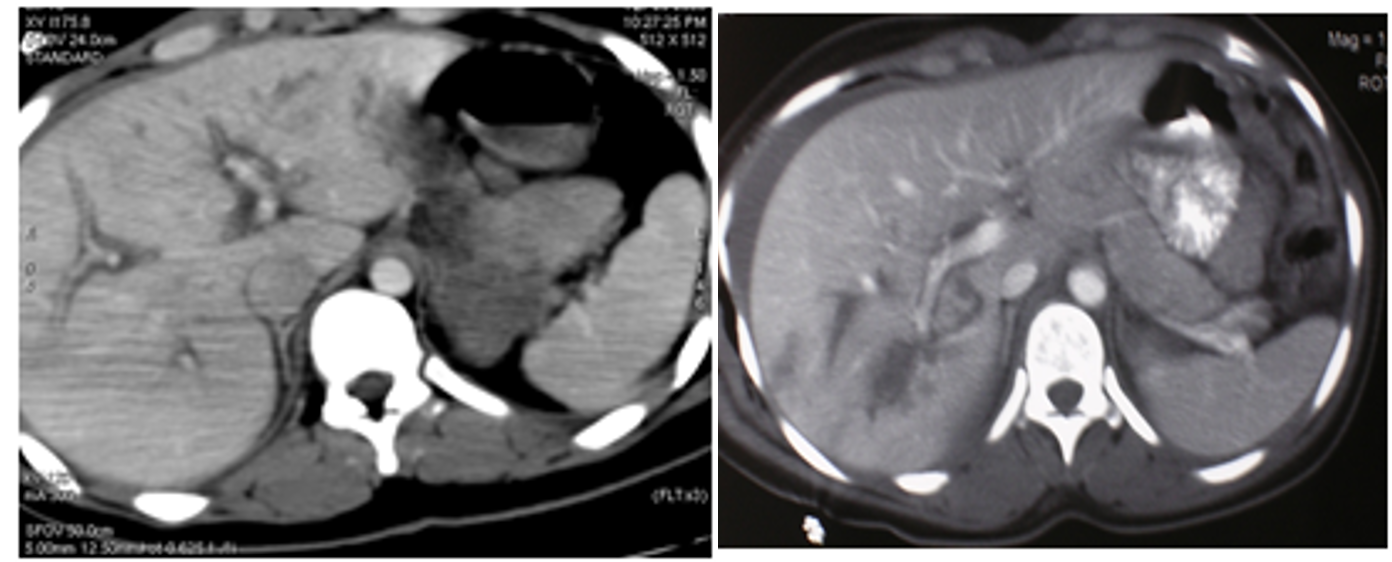
Diagnosis:
- Hemodynamically unstable- FAST
- Hemodynamically stable- FAST, CT scan
- Management based on hemodynamic status
(Image: Liver injury- CT scan)
Liver injury- Non-operative management
- Hemodynamically stable patients
- CT scan
- If No other indications for abdominal exploration
- ICU admission for close observation
- Serial hemoglobin estimation
- Transfusion requirements of <2 units of blood
- Surgery- if become unstable
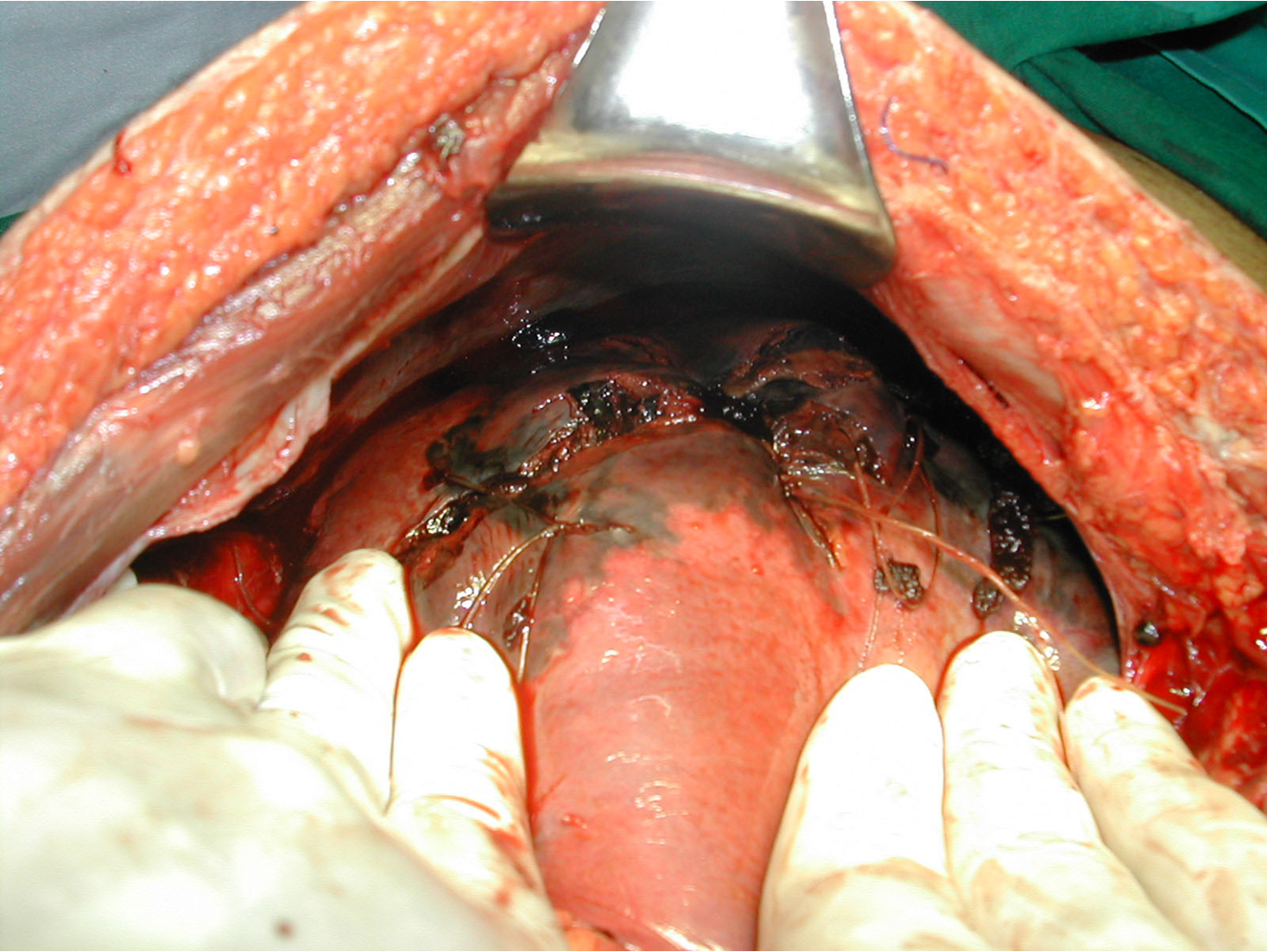
Liver injury-Surgical management
Principles of surgical management:
- control of bleeding,
- removal of devitalized tissue, and
- adequate drainage.
-
Bleeding vessels & biliary radicles are individually ligated.
-
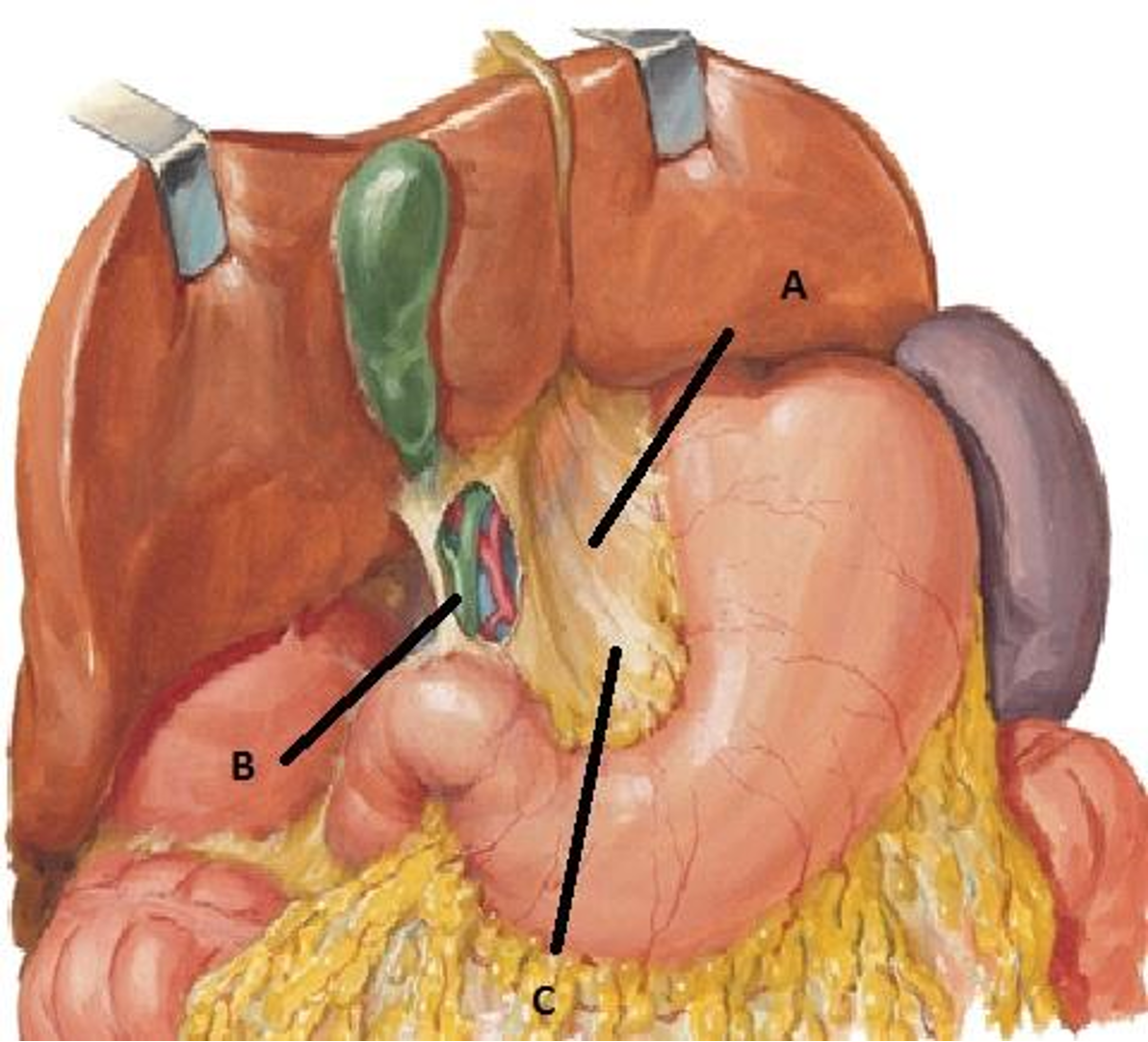
Pringle’s maneuver: clamping the hepatoduodenal ligament (the free border of the lesser omentum)
-
Perihepatic packing- if fail to control bleeding.
-
Packs removed in 48 hours.