Pediatrics
HYDROCEPHALUS
Definition:
Excessive volume of intracranial cerebrospinal fluid causing ventricular dilatation.
Three main categories for pathophysiology:
- Increase production of CSF
- Obstruction in CSF Flow tract
- Decrease Absorption of CSF
Remember:
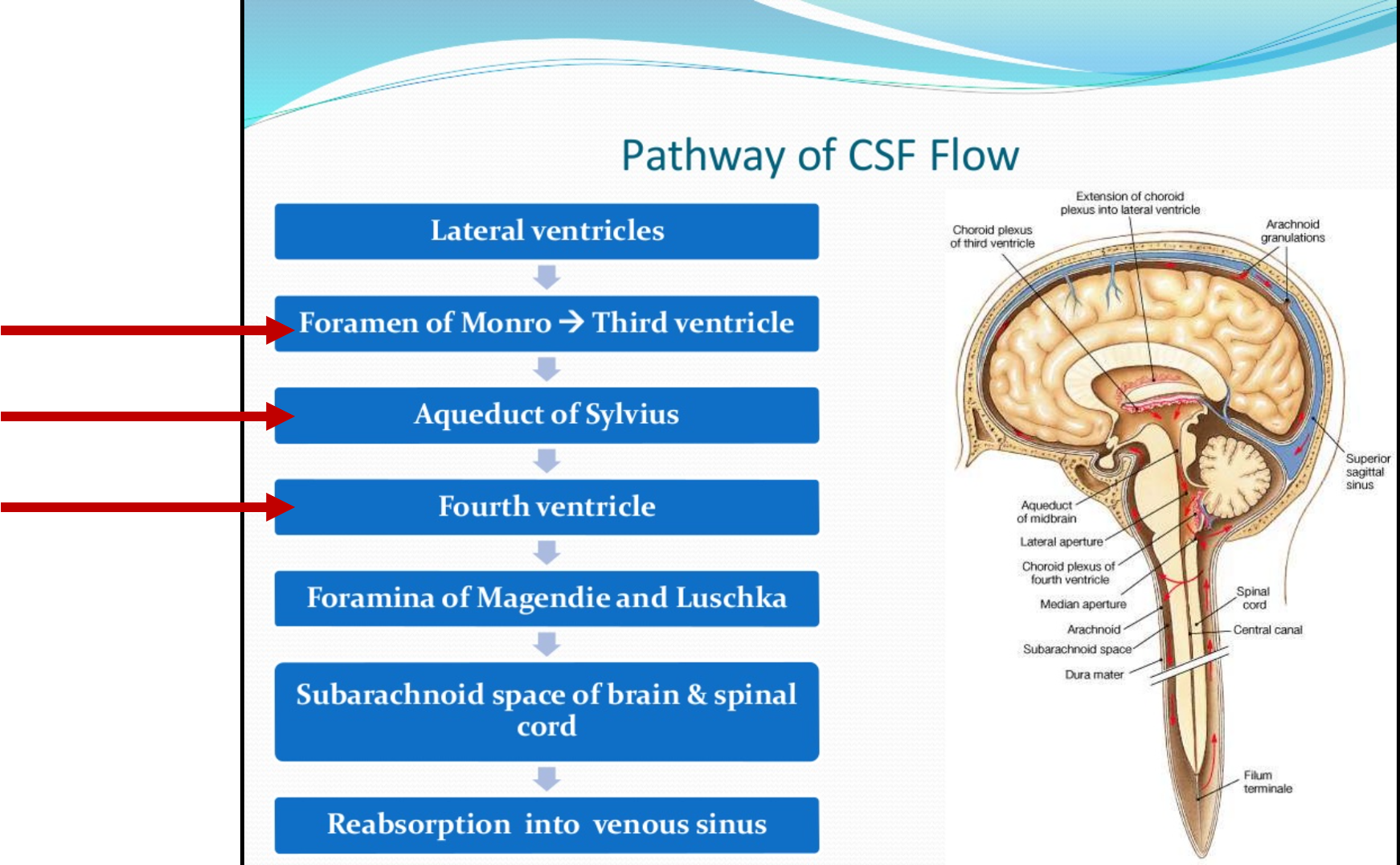
- CSF is produced in choroid plexus & spinal subarachnoid space (400-500 ml per day)
- CSF is absorbed in arachnoid granulations
Obstructive (noncommunicating) hydrocephalus
Type of hydrocephalus in which there is blockage somewhere in ventricular system causing accumulation of CSF
Causes of obstructive hydrocephalus Acquired:
- Posterior fossa tumor (These patients will present with ataxia, papilledema, headache)
- Intraventricular clot
- Abscess (tb, fungal, heart defects)
- Intraventricular hemorrhage (common in low birth preterm)
Congenital:
- Congenital aqueduct stenosis
- Dandy walker malformation
Non-Obstructive (communicating)
Type of hydrocephalus in which there is either abnormality in CSF absorption (which occurs at Arachnoid granulations) or overproduction of CSF.
CSF is freely flowing between ventricles and subarachnoid space.
Causes of impaired CSF absorption
- Meningitis
- Example: CMV, Toxoplasmosis, TB, Bacterial
- Subarachnoid hemorrhage
- Intraventricular hemorrhage (common in low birth preterm)
- Metabolic conditions
Management: treat based on the cause
Causes of excessive CSF production
- Choroid plexus papilloma
- Carcinoma
Management:
- Surgical Removal
- Posthemorrhagic hydrocephalus may occur post-surgical removal due to high nature of blood vessels of these tumors.
- Serial X-ray follow-ups along with permanent shunting will be required.
Signs and symptoms of hydrocephalus
Symptoms:
- Decrease in activity or irritability
- Lethargy
- Drowsiness
- Poor feeding
- Poor weight gain
Most common symptom in older children is: early morning headache with vomiting
Signs (neonates):
- Excessive head growth rapidly crossing percentiles
- Frontal bossing
- Tense anterior fontanelle (meningitis/sepsis participating factors)
- Dilated scalp veins
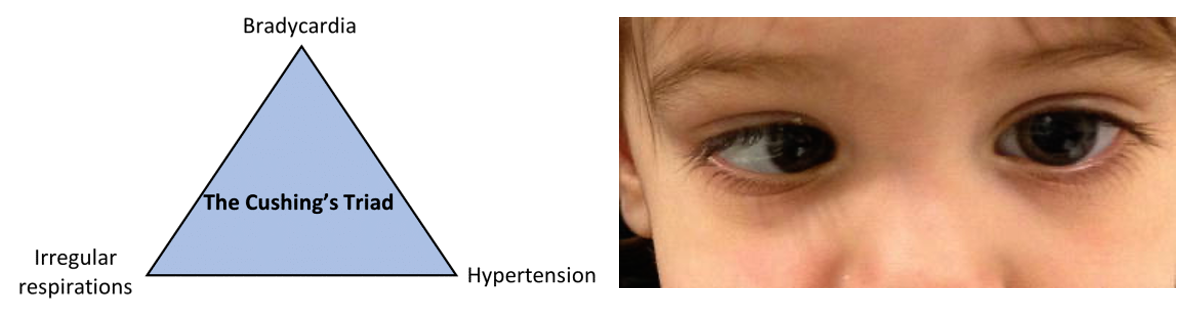
- Sun-set eyes

Signs (older children):
- Hyperreflexia
- Hypertonia
- Developmental Delay
- Sixth nerve palsy
- Cushing Triad (presenting high intracranial pressure)
Management
Initially, patients should have regular follow-up for serial head measurements and plot it on growth chart to make diagnosis.
Brain US through anterior fontanel for infants and MRI for older children are done to confirm hydrocephalus.
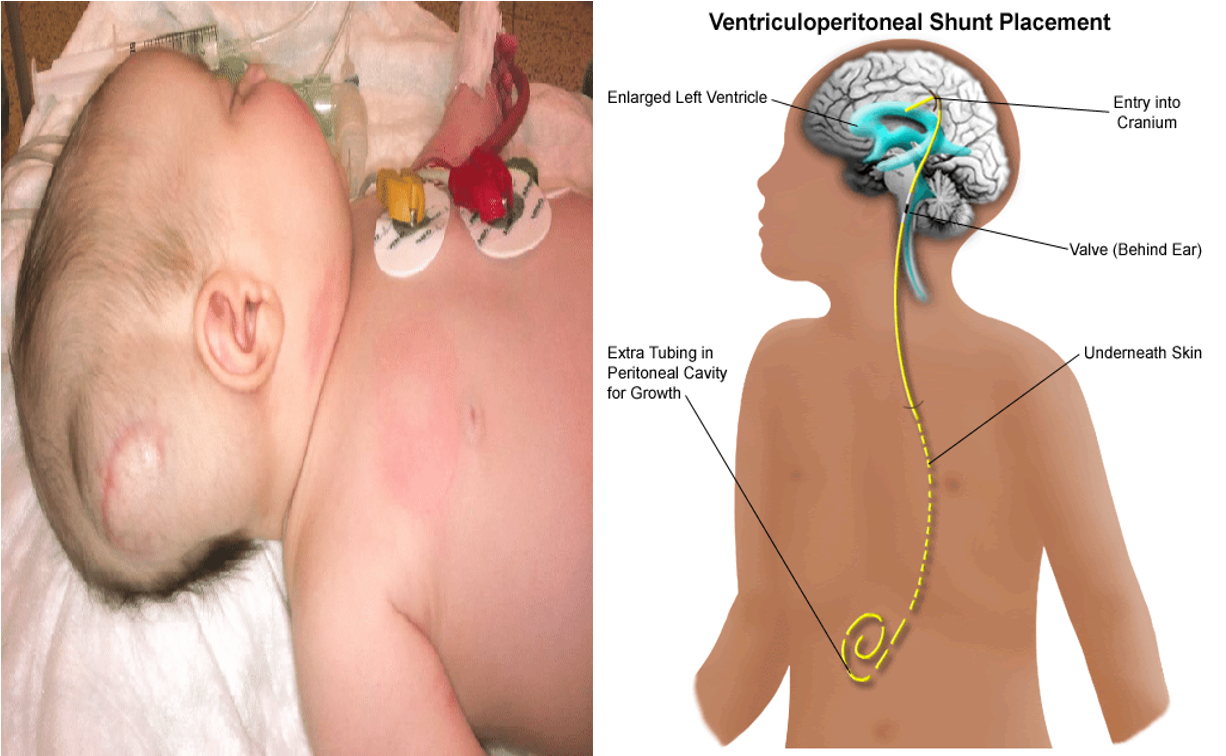
Ventriculoperitoneal Shunting is the main treatment for hydrocephalus.
Parent’s counseling should be offered every clinic visit to observe for any early signs of VP malfunction.
Complications of VP Shunt
-
Ventriculitis
-
Patient will present with fever and seizures. If VP shunt malfunctions, hydrocephalus signs will also be seen.
Most common organism:
Staphylococcus Epidermidis
- Vancomycin
Radiology
Cause elevated intracranial pressure (ICP), which leads to headache, nausea, and/or vomiting.
Ultrasonography
-
Indication: clinical suspicion during antenatal period or in infants < 18 months of age (through the anterior fontanelle when it is still open)
-
Findings: enlarged lateral ventricles
MRI or CT
-
Children > 18 months of age (fontanelle is already closed) and adults.
-
Communicating hydrocephalus: all ventricles are dilated
-
Noncommunicating hydrocephalus: ventricles upstream of the obstruction are dilated
-
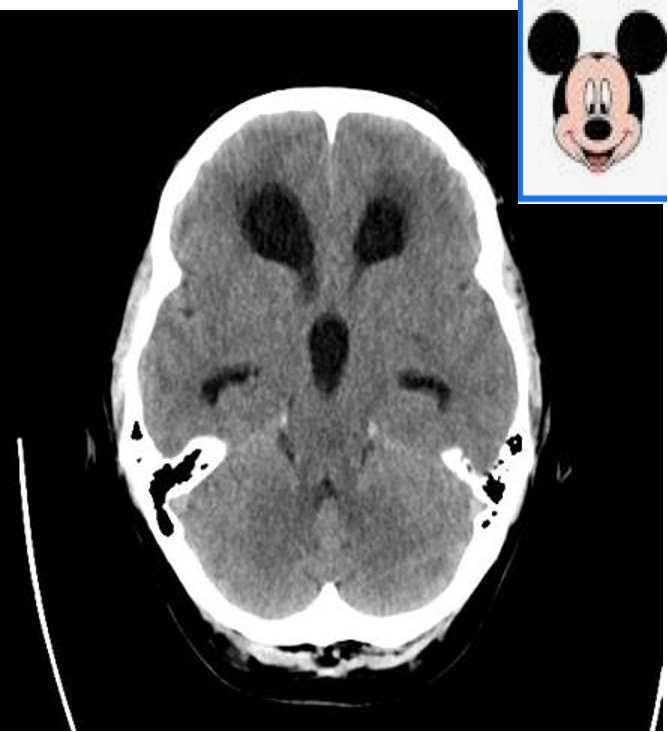
Features of acute hydrocephalus
-
Enlarged ventricles
- Temporal horn dilation > 2 mm
- Mickey Mouse ventricles (enlarged lateral and third ventricle)
- Sulcal enlargement.
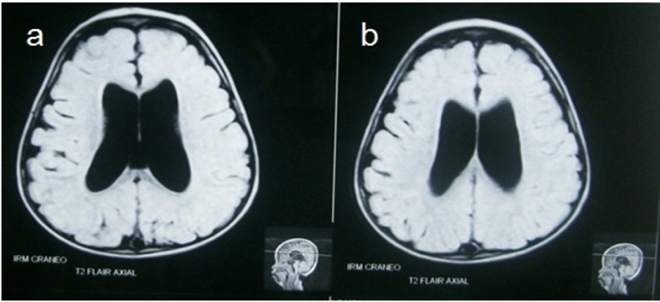
MRI head (FLAIR sequence; two axial planes)
of a young child with Dilated lateral ventricles are seen in the center of both images.
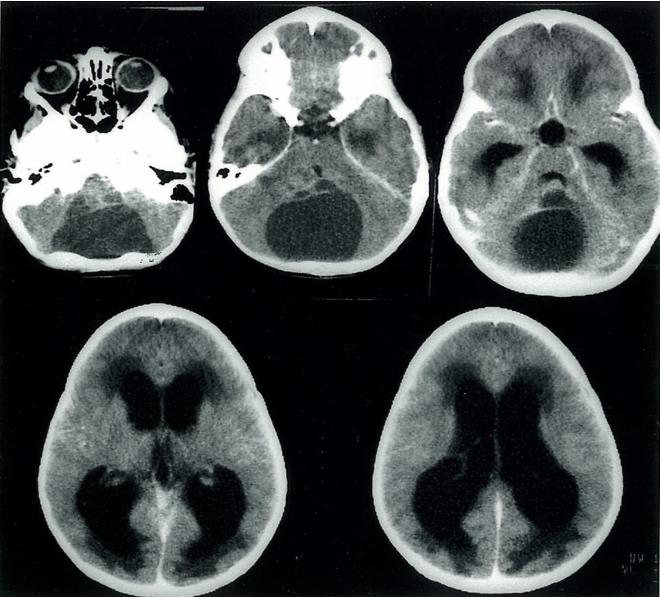
Noncommunicating hydrocephalus Cranial CT (axial view) of a 13-year-old boy
A large, liquor-like, hypodense lesion is located in the posterior cranial fossa in images 1–3. This lesion is most likely an arachnoid cyst compressing the cerebral aqueduct), which prevents the free circulation of the CSF from the ventricles to the subarachnoid space. As a result, the third ventricle and the lateral ventricles are dilated, and there is transependymal egress of CSF
Cranial CT (axial view)
Significant enlargement of the lateral ventricles. The anterior falx cerebri appears hyperdense due to calcification.
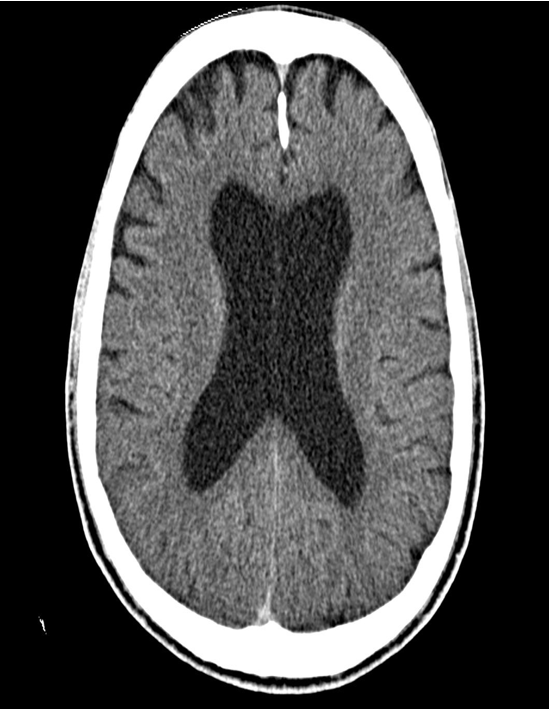
Hydrocephalus:
Third and both lateral ventricles are dilated but the fourth ventricle is normal. It shows that the Obstruction is above the level of fourth ventricle. In this case blockage is in the aqueduct.