Development and Behavior
Dr. Faten Zaidan
Factors to be Considered While Assessing Development
| Table 8.4: Context of Behavioral Problems |
|---|
| Child Factors |
| Health (past and current) |
| Developmental status |
| Temperament (e.g., difficult, slow to warm up) |
| Coping mechanisms |
| Parental Factors |
| Misinterpretations of stage-related behaviors |
| Mismatch of parental expectations and characteristics of child |
| Mismatch of personality style between parent and child |
| Parental characteristics (e.g., depression, lack of interest, rejection, overprotective, coping) |
| Environmental Factors |
| Stress (e.g., marital discord, unemployment, personal loss, perceived racism) |
| Support (e.g., emotional, material, informational, child care) |
| Poverty—including poor housing, poorer education facilities, lack of access to healthy foods (food deserts), unsafe environments, toxic stress, poor access to primary care |
| Racism |
Definition of Normal Development:
Parallel to the changes in the developing brain (i.e., cognition, language, behavior) are changes in the physical development of the body.
The History
Screening is Based on the:
- History
- Physical and developmental examination
- Interpretation and comparison to normal child at the same age
General History:
- Birth weight and duration of gestation.
- Prenatal risk factors e.g., infectious, hypertension.
- Genetic factors: mental subnormality.
- Familial pattern of development.
- Perinatal factors e.g., fetal distress.
Condition at birth.
- Postnatal development e.g., when beginning to smile. Sucking or swallowing difficulties, irritability, etc.
- Major illnesses, emotional deprivation, etc.
- The previous development: Is he showing accelerated development? or slowing of development (i.e., loss of attained functions) e.g., neurodegenerative diseases?
Developmental History:
- Assess the mother’s understanding and memory.
- Ask whether the baby shows a particular skill (e.g., smiles) and when he began to show it.
Examination of Primitive Reflexes
Examination of the primitive reflexes provides assessment of the functional integrity of the brainstem and basal ganglia, indicating the normal maturation of descending inhibitory cerebral influences. Asymmetry or persistence of the primitive reflexes may indicate focal brain or peripheral nerve lesions.
| REFLEX | DESCRIPTION | AGE AT APPEARANCE | AGE AT DISAPPEARANCE |
|---|---|---|---|
| Moro | Light drop of head produces sudden extension followed by flexion of the arms and legs | Birth | 3–6mo |
| Grasp | Placing finger in palm results in flexing of infant’s fingers | Birth | 3–4mo |
| Rooting | Tactile stimulus at the side of the mouth causes the mouth to pursue the stimulus | Birth | 3–4mo |
| Trunk incurvation (Gallant) | Stroking the skin along the edge of vertebrae produces curvature of the spine with concavity on the side of the stimulus | Birth | 4mo |
| Placing | When dorsum of foot is brought into contact with the edge of a surface, infant places foot on the surface | Birth | 4–6mo |
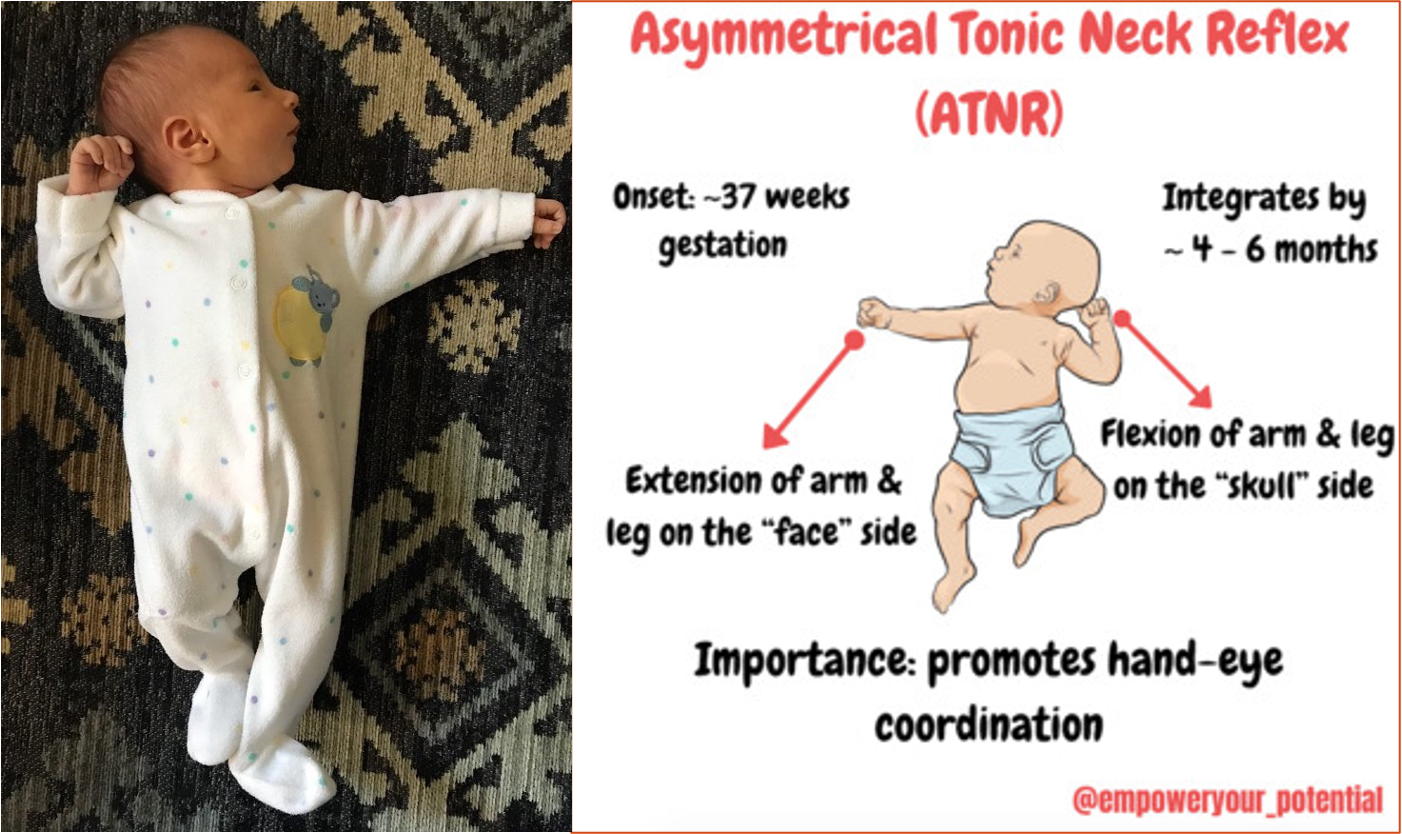
| Asymmetric tonic neck | With infant supine, turning of the head results in ipsilateral extension of the arm and leg with flexion of opposite extremities in a “fencing” posture | Birth | 3mo |
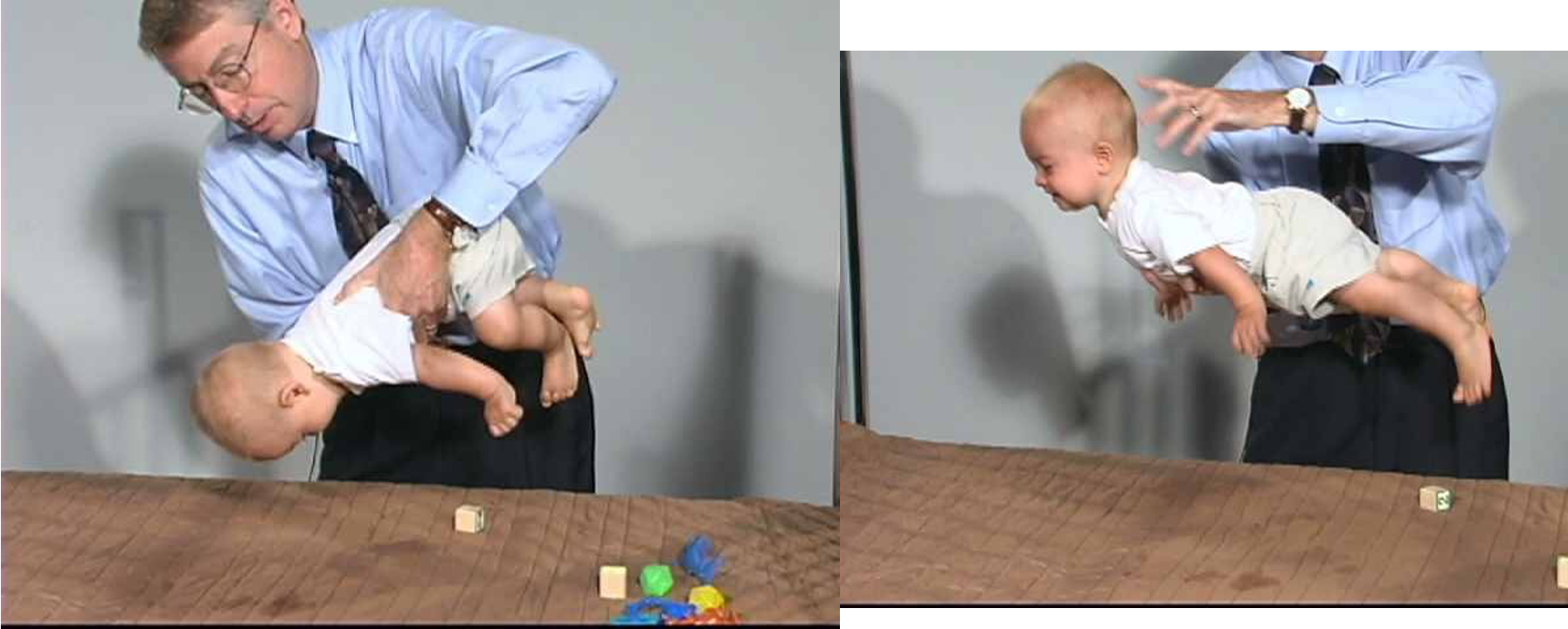
| Parachute | Infant is suspended face down by the chest. When infant is moved toward a table, the arms extend as if to protect self | 8–10mo | Never |
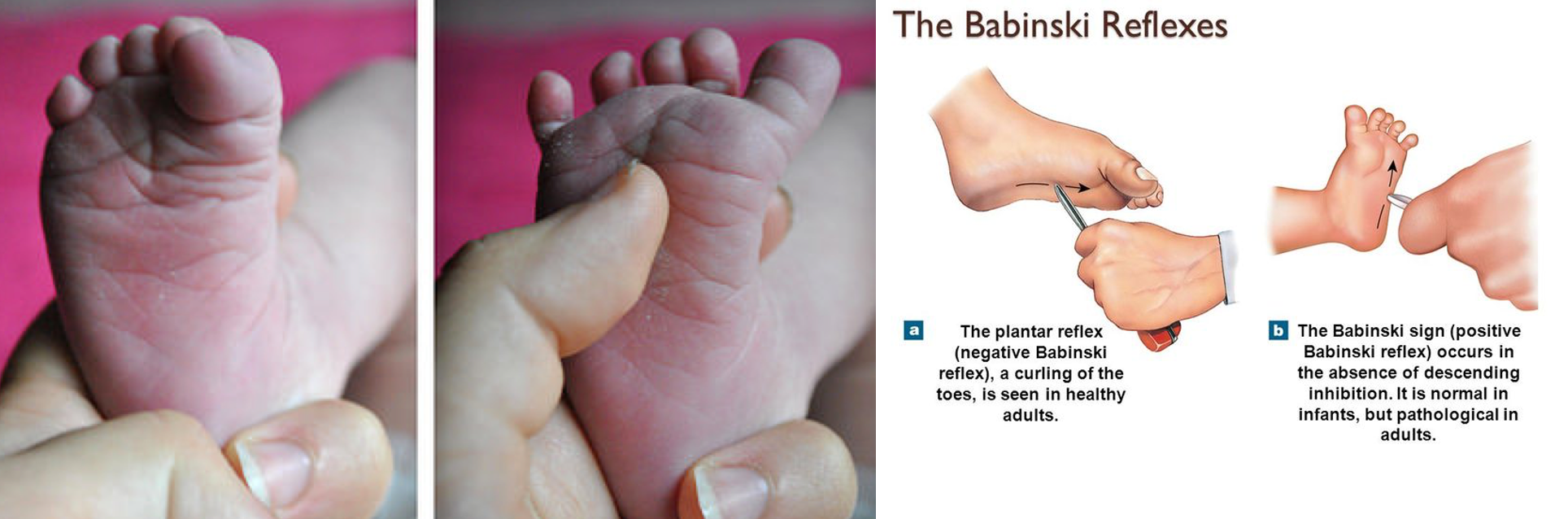
| Babinski | Stroking lateral aspect of sole from heel up results in dorsiflexion of the great toe and fanning of the remaining toes | Birth | 12–18mo |
Moro Reflex
The Moro reflex is elicited by allowing the infant’s head to gently move back suddenly (from a few inches off of the mattress onto the examiner’s hand), resulting in a startle, then abduction and upward movement of the arms followed by adduction and flexion. The legs respond with flexion.

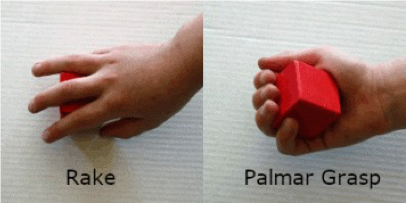
Grasp Reflex

Rooting Reflex
The rooting reflex is elicited by touching the corner of the infant’s mouth, resulting in lowering of the lower lip on the same side with tongue movement toward the stimulus. The face also turns toward the stimulus.

Gallant Reflex

Placing Reflex

Asymmetric Tonic Neck Reflex
The asymmetric tonic neck reflex is elicited by placing the infant supine and turning the head to the side. This placement results in ipsilateral extension of the arm and the leg into a “fencing” position. The contralateral side flexes as well.
Parachute Reflex
Babinski Reflex
Sucking Reflex
The sucking reflex occurs with almost any object placed in the newborn’s mouth. The infant responds with vigorous sucking. The sucking reflex is replaced later by voluntary sucking.

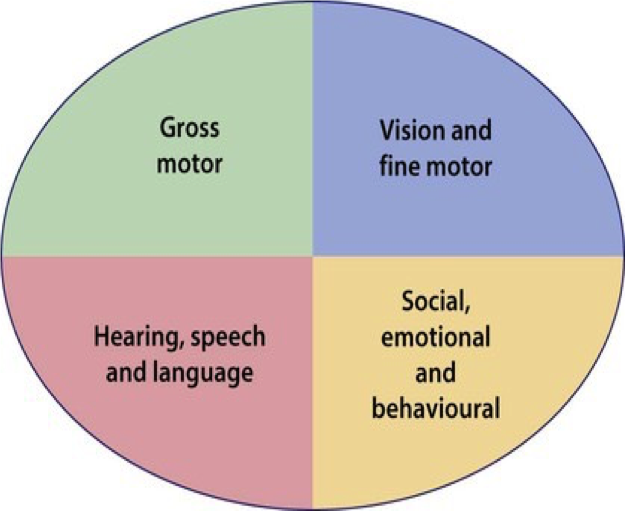
Development Milestones
Here’s the table in text format:
| Age | Gross Motor | Fine Motor–Adaptive | Personal-Social | Language |
|---|---|---|---|---|
| 2 wk | Moves head side to side | — | Regards face | Alerts to bell |
| 2 mo | Lifts shoulder while prone | Tracks light past midline | Smiles responsively | Cooing Searches for sound with eyes |
| 4 mo | Lifts up on hands Rolls front to back If pulled to sit from supine, no head lag | Reaches for object Raking grasp | Looks at hand Begins to work toward toy | Laughs and squeals |
| 6 mo | Sits alone Rolls back to front | Transfers object hand to hand | Feeds self Holds bottle | Babbles |
| 9 mo | Pulls to stand Gets into sitting position | Starting to pincer grasp Bangs two blocks together | Waves bye-bye Plays pat-a-cake | Says Dada and Mama, but nonspecific Two-syllable sounds |
| 12 mo | Walks Stoops and stands | Puts block in cup | Drinks from a cup Imitates others | Says Mama and Dada, specific Says one to two other words |
| 15 mo | Walks backward Stoops and recovers | Scribbles Stacks two blocks | Uses spoon and fork Helps in housework | Says three to six words Follows commands |
| 15 mo | Walks backward Stoops and recovers | Scribbles Stacks two blocks | Uses spoon and fork Helps in housework | Says three to six words Follows commands |
| 18 mo | Runs | Stacks four blocks Kicks a ball | Removes garment “Feeds” doll | Says at least six words |
| 2 yr | Walks up and down stairs Throws overhand | Stacks six blocks Copies line | Washes and dries hands Brushes teeth Puts on clothes with assistance | Puts two words together Points to pictures Knows body parts |
| 3 yr | Walks steps alternating feet Broad jump | Stacks eight blocks Wiggles thumb | Uses spoon well, spilling little Puts on T-shirt | Names pictures Speech understandable to stranger 75% Says three-word sentences |
| 4 yr | Balances well on each foot Hops on one foot | Copies O, maybe + Draws person with three parts | Brushes teeth without help Dresses without help | Names colors Understands adjectives |
| 5 yr | Skips Heel-to-toe walks | Copies □ | — | Counts Understands opposites |
| 6 yr | Balances on each foot 6 sec | Copies △ Draws person with six parts | — | Defines words |
4 Months Old
10 Months old

Following objects
- 1 month: follows to midline
- 2 months: follows past midline
- 3 months: follows 180°
Language: expressive - Speech and Language
- Coos
- 2 months (2–4 months)
- Laughs out loud
- 4 months
- Babbles
- 6 months
- Mama or dada nonspecific
- 9 months
- Mama and dada specific
- 12 months
- Vocabulary of 10–25 words
- 18 months
- Two-word sentences
- 2 years (18–24 months)
- Three-word sentences
- 3 years (2–3 years)
- Four-word sentences
- 4 years (3–4 years)
Cubes
Blocks
- Passes cubes
- More than 6 months
- Bangs cubes
- 9 months
- Block in a cup
- 12 months
- Tower three blocks
- 15 months
- Tower four blocks
- 18 months
- Tower six blocks
- 24 months
- Bridge from blocks
- 3 years
- Gate from blocks
- 4 years
- Steps from blocks
- 5 years

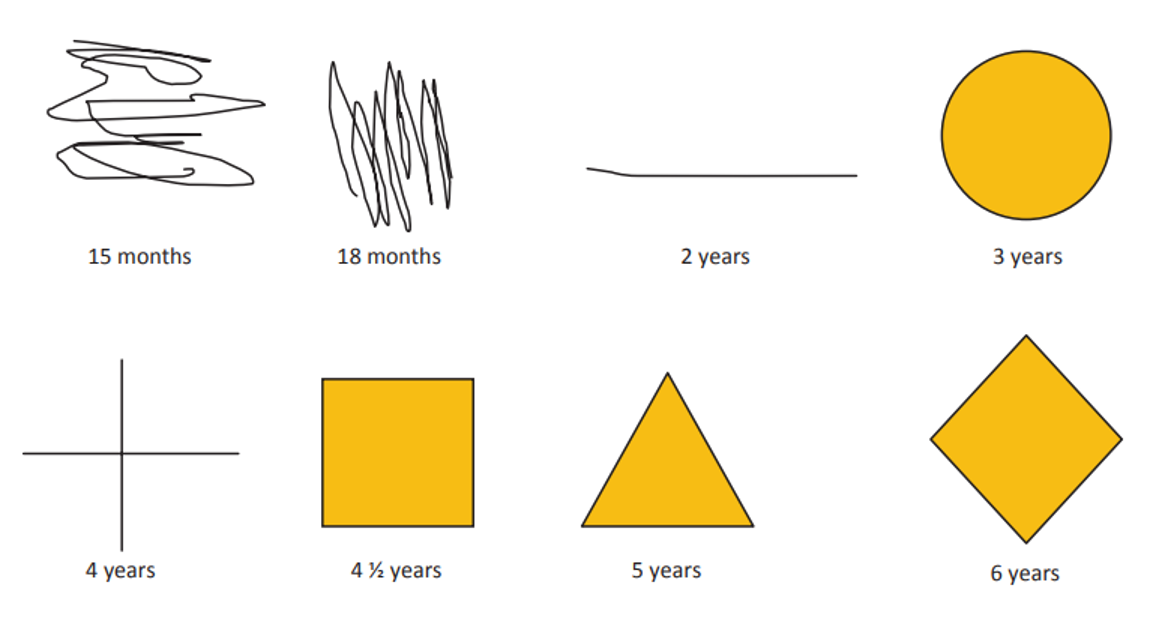
Drawing
Drawing
- Scribbles
- 15 months
- Circle
- 3 years
- Cross
- 4 years
- Square
- 4.5 years
- Triangle
- 5 years
- Diamond
- 6 years
Red Flags in Development as per Age
| Age | Red Flags |
|---|---|
| 2 months | Lack of fixation *** |
| 4 months | Lack of visual tracking |
| 6 months | Failure to turn to sound or voice *** |
| 9 months | Lack of babbling consonant sounds |
| 24 months | Failure to use single words, cannot follow simple direction, pointing instead of speaking |
| 3 years | Failure to speak in three-word sentences *** |
| 4 years | Cannot tell story |
Cause of language developmental delay
- Hearing impairment
- Intellectual disability
- Autism
- Specific language disorders
- Dysarthria
- Dyspraxia
- Maturation delay
- Neglect
Bicycle & Scooter
- 3-wheels bicycle: 3 years old
- 2-wheels bicycle with training wheels: 4 years old
- 2-wheels bicycle without training wheels: 5 years old
- 3-wheels scooter: 4 years old
- 2-wheels scooter: 5 years old

Stairs
A) Going Up:
- 18 months old: Two feet on each step with support
- 2 years old: Two feet on each step without support
- 3 years old: One foot on each step
B) Going Down:
- 2 years old: 2 feet on each step
- 3 years old: One foot on each step without support