Brachial Plexus Injuries
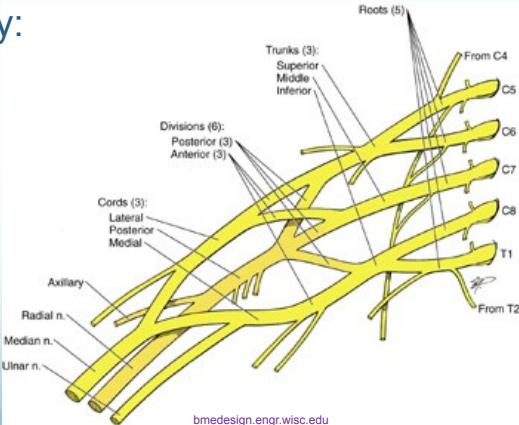
Anatomy and Structure
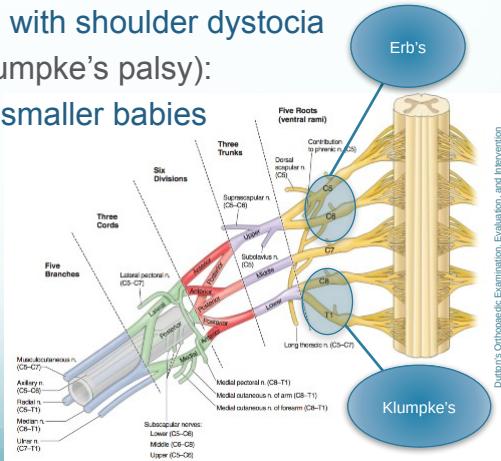
- Origin: Brachial plexus originates from C5-C8 and T1 spinal nerve roots
- Organization: Complex network of nerves that provides innervation to the upper extremity
Mechanisms of Injury
- Compression: External pressure on the plexus
- Stretch/Traction: Forces that pull the nerve roots
- Laceration: Sharp or penetrating injuries
- Avulsion: Tearing of nerve roots from spinal cord
Etiology
- Traumatic injuries:
- High-speed vehicular accidents
- Stab or gunshot wounds
- Severe shoulder trauma
- Obstetric injuries:
- Difficult delivery procedures
- Shoulder dystocia complications
- Compression causes:
- Growing tumors (e.g., Pancoast tumor)
- Chronic pressure syndromes
Classification and Types
Injury Severity Patterns
- Overstretching injuries:
- Nerve roots remain intact
- May involve intact axons (neuropraxia) or cut axons (axonotmesis)
- Rupture injuries:
- Nerve roots stretched and partially torn
- Mixed recovery potential depending on severity
- Avulsion injuries:
- Nerve roots pulled out from spinal cord
- No chance for spontaneous recovery
Prognosis by Injury Type
| Injury Type | Recovery Prognosis | Clinical Course |
|---|---|---|
| Neuropraxia | Excellent | Complete recovery expected |
| Axonotmesis | Moderate | Good but may have residual deficits |
| Neurotmesis/Avulsion | Poor | Very limited recovery without surgery |
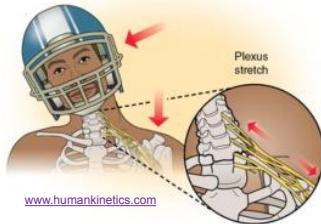
Source: www.humankinetics.com

Source: en.wikipedia.org
Brachial Plexus Palsy Syndromes
Obstetric Brachial Plexus Palsy
Epidemiology:
- Occurs in <1% of live births
- Most commonly associated with shoulder dystocia during delivery
- Risk factors include large birth weight and difficult delivery
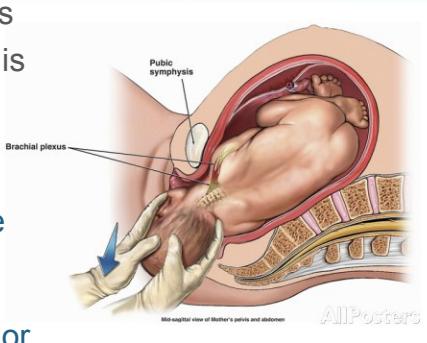
Pathophysiology:
- Baby’s shoulder becomes impacted on mother’s pubic bone
- Brachial plexus nerves undergo stretch or tear injuries
- Injury severity depends on traction forces and duration
Clinical Patterns
Three main patterns of brachial plexus palsy:
-
Upper Root Injury (Erb’s Palsy):
- Roots involved: C5-C6 (sometimes C7)
- Typical scenario: Overweight babies with shoulder dystocia
- Clinical presentation: “Waiter tip position”
-
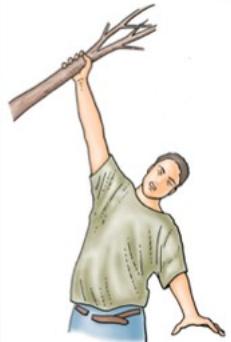
Lower Root Injury (Klumpke’s Palsy):
- Roots involved: C8-T1
- Typical scenario: Breech delivery of smaller babies
- Clinical presentation: Intrinsic hand muscle weakness
-
Total Plexus Injury:
- Roots involved: C5-T1 (entire plexus)
- Most severe form with complete upper extremity dysfunction
Erb’s Palsy (Upper Root Injury)
Nerve Roots Involved:
- Primary: C5-C6
- May extend to: C7 in more severe cases
Muscle Groups Affected:
- Shoulder abductors (deltoid, supraspinatus)
- Shoulder external rotators (infraspinatus, teres minor)
- Elbow flexors (biceps brachii, brachialis)
- Supinators (supinator, biceps)
Clinical Presentation:
- Classic “Waiter Tip Position”:
- Arm held adducted to the side
- Internally rotated shoulder
- Extended elbow
- Pronated forearm
- Motor function: Weakness in shoulder abduction and elbow flexion
- Sensory function: Usually preserved over lateral arm

Klumpke’s Palsy (Lower Root Injury)
Nerve Roots Involved:
- Primary: C8-T1
- Affects: Ulnar and median nerve distribution
Mechanisms of Injury:
- Traction injuries from excessive arm abduction
- Common causes:
- Falls from height with arm outstretched
- Cervical rib anatomical variant
- Violent upward traction
Motor Manifestations:
- Intrinsic hand muscles: Complete paralysis
- Wrist flexors: Variable weakness
- Fine motor skills: Severely compromised
Sensory Manifestations:
- Distribution: Loss along medial forearm and hand
- Key areas: Medial arm, medial forearm, little finger side of hand
Characteristic Deformity:
- Claw hand deformity:
- Extended MCP joints
- Flexed IP joints
- Prominent metacarpal heads
- Ulnar deviation



Total Plexus Injury
Clinical Features:
- Complete flail limb: No active movement in entire upper extremity
- Skin changes: Pale, cool extremity due to loss of sympathetic tone
- Complete sensory loss: No sensation throughout the arm
- Motor paralysis: All muscles of upper extremity affected
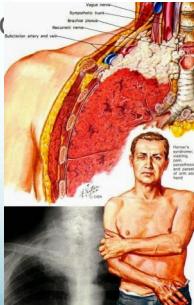
Associated Findings:
- Horner’s syndrome (indicative of proximal root avulsion):
- Ptosis: Drooping of upper eyelid
- Miosis: Constriction of pupil
- Enophthalmos: Sunken appearance of eyeball
- Anhydrosis: Absence of sweating on affected side

Source: www.riversideonline.com