Axillary Nerve Injury
Anatomy
Origin:
- Nerve roots: C5-C6
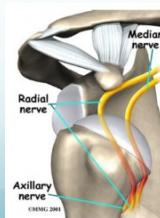
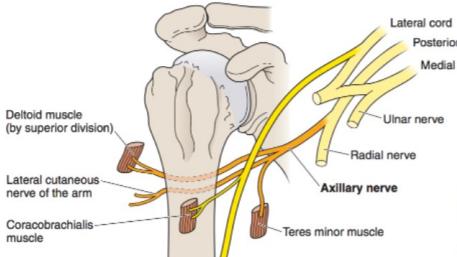
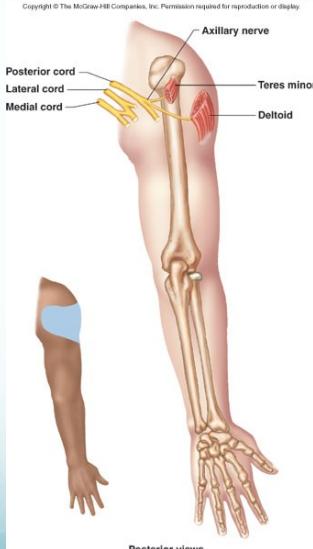
- Branches from: Posterior cord of brachial plexus
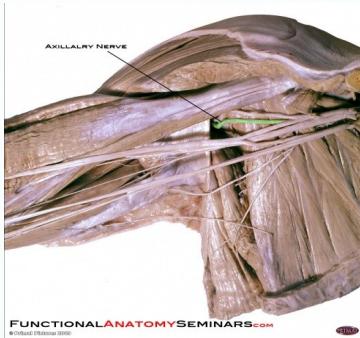
- Location: Axilla region
Course and Distribution:
- Travels through quadrangular space with posterior humeral circumflex artery
- Winds around surgical neck of humerus
- Supplies deltoid region and teres minor
Common Injury Mechanisms
- Anterior-inferior shoulder dislocations: Most common cause
- Surgical neck fractures of humerus: Direct nerve injury or compression
- Improper crutch use: Prolonged compression in axilla
- Direct trauma: Blunt injuries to shoulder region
Innervation Pattern
Motor Innervation
- Deltoid muscle: Primary shoulder abductor
- Teres minor: Shoulder external rotator
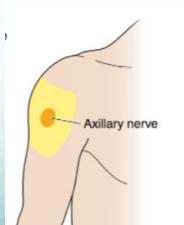
Sensory Innervation
- Superior lateral cutaneous nerve of arm:
- Skin over inferior (“badge”) region of deltoid
- Small area on lateral aspect of upper arm
Clinical Presentation
Motor Deficits
- Shoulder abduction weakness: Loss of deltoid function beyond 90°
- External rotation weakness: Teres minor involvement
- Visible muscle wasting: Deltoid atrophy over time
Physical Signs
- Flat shoulder deformity: Loss of deltoid contour
- Limited arm abduction: Cannot maintain arm in abducted position
- Compensatory movements: Uses shrugging or trunk leaning
Sensory Deficits
- Loss of sensation: Small patch over lateral upper arm
- Often minimal: Sensory loss may be clinically insignificant
Diagnostic Testing
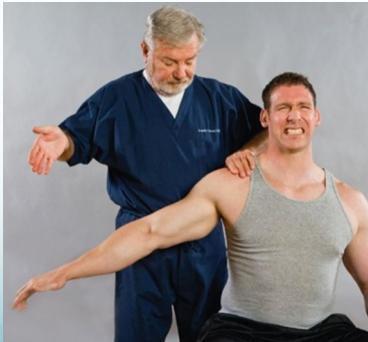
Arm Drop Test (Deltoid Test)
Procedure:
- Patient stands with arm at side
- Examiner passively abducts arm to approximately 90°
- Patient asked to actively maintain position
- Examiner releases support
Positive Test Result:
- Arm drops from abducted position
- Inability to maintain shoulder abduction
- Indicates: Deltoid weakness/paralysis
Clinical Significance:
- Highly specific for axillary nerve dysfunction
- Distinguishes from supraspinatus lesions