A 5-year-old boy, presented with history of fatigue and weakness.
The family originally from the south province of kingdom and parents are first cousins.
Clinical examination. The child’s weight was 13.9 kg ( below 3rd percentile ),height 109.5 cm (50th percentile) and her head circumference was 54 cm( above 97th percentile).
Markedly pale and also had mild clinical jaundice. Temp: 37.2, P 100, R 30, BP 98/52. He is nontoxic appearing. Lungs are clear to auscultation. Heart is regular with short systolic murmur grade 2/6 at ULSB. Signs of extramedullary erythropoiesis were present, notably frontal bossing and maxillary hyperplasia .
No significant lymphadenopathy.
-
a- Write two relevant questions, to ask the mother.
-
b- Mention 2 important specific signs you should look for during examination of this child.
-
c- Write two important investigations.
-
d- What is the most likely diagnosis and give two differential diagnosis? B. thalacemia major
-
e- Mention two important points in the management. plan
4months old baby had a cough and on examination he had expiratory wheezing and fine crepitation.
- 2 relevant questions in history
- Sings in examination
- Investigations
- Diagnosis and differential diagnosis
- Treatment
9 y/o female. Has twitches in her arms and mouth and migratory polyarthralgia(knee, ankle, elbow) one month ago, the pain relieved after taking aspirin. She has no fever. CVS examination shows systolic murmur.
- 3 relevant questions in history
- Sings in examination
- Investigations
- Diagnosis and differential diagnosis
- Treatment
- Anterio-posterior [AP] chest radiograph shows multiple cystic lesions in– (1 -the middle and lower zones of the left hemi-thorax with ill-defined left hemi diaphragm. There is mediastinal shift toward the right. These lesions are -bowel loops inside the left hemi-thorax. The film is over exposed (over .(penetration
- The diagnosis is Left Sided Congenital Diaphragmatic Hernia (CDH). This - (2 is called bockdalic CDH. CDH is usually in the left side (90 %). The defect is found in the posterio-lateral aspect of the diaphragm. CDH is associated with .lungs hypoplasia in the same side and to a lesser extent in the opposite side .This may be complicated by pulmonary hypertension and severe hypoxemia
- The treatment of CDH is immediate endo-tracheal incubation if it is - (3 diagnosed in-utero or if it is highly suspected after birth (with following symptoms and; respiratory distress (RD), cyanosis, asymmetrical chest movement, bowel sounds heard in the chest and scaphoid abdomen). After intubation, the patients is put on mechanical ventilator and the pulmonary hypertension [PH] is controlled and hypoxemia is reversed. PH and severe hypoxemia may require inhaled Nitric Oxide [iNO], High frequency Oscillatory Ventilation [HFOV] and Exogenous Surfactant administration through endotracheal tube [ETT]. After the stabilization of the arterial blood gases the patient is taken to suture the defect. If the defect is large, a mesh,[ABGs] device may be used. The most important differential diagnosis is Cystic .Adenomatoid Malformation [CAM]
- AP chest film showing that the naso-gastric tube (NGT) is inside the left - (1 hemi-thorax. There is an ill-defined line separating the upper and middle .zones of left lung
- The diagnosis was ruptured left hemi-diaphragm possibly secondary to - (2 .the trauma to the abdomen
- During surgery, there was a ruptured diaphragm and intestines, spleen - (3 and stomach were found in the left chest. There was evidence of left sided .CDH which facilitated the rupture
- The abdominal X-ray shows a hyper-lucent shadow separating the liver - (1 from the abdominal wall. This represents free air in the abdomen .which results from intestinal perforation (pneumoperitoneum)
- .The cause of perforation is early and rapid feeding after cardiac arrest - (2 .Intestinal ischemia after cardiac arrest needs time to resolve
- This complication can be prevented by delaying the feed till 7 days elapse - (3 .from the arrest and upgrading the feed gradually
- This X-ray is a lateral view of the legs showing severe osteopenia and - (1 spiral fracture in the middle of the tibia. There are signs of rickets in .the metaphyses such as cupping in both knee and ankle joint
- The cause is Osteopenia Of Prematurity [OOP] found in premature - (2 babies. It is similar to rickets. The causes are; calcium, phosphorus and Vitamin D deficiencies. The fracture can occur with mild twisting of the legs during attempt to insert an intra-venous access. The treatment is .supplementation with Calcium, Phosphorus and Vitamin D
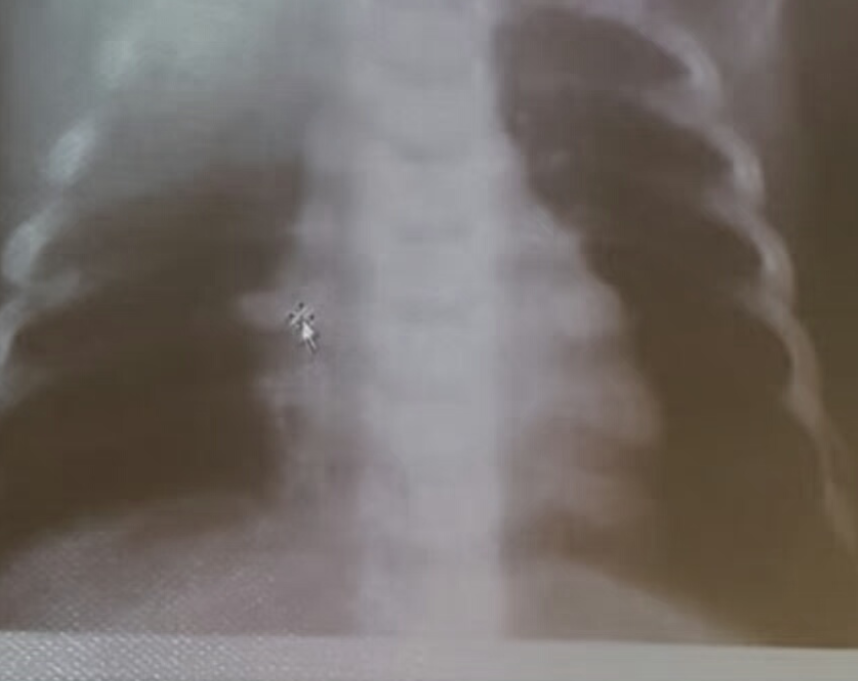
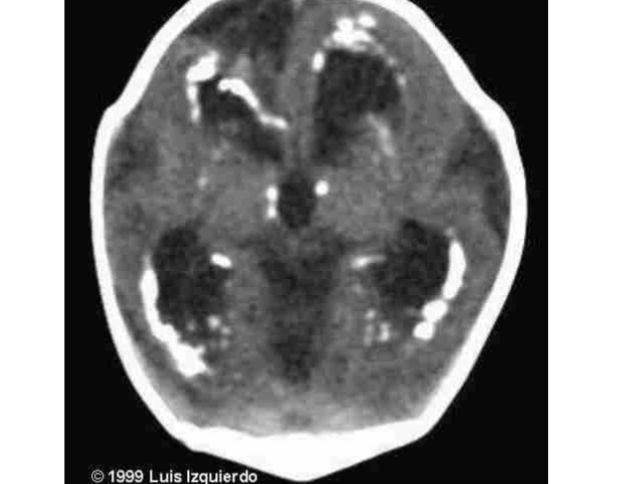
- ,There is symmetrical, bilateral, hyper-dense (whitish), rounded lesions - (1 :approximately 1.5 × 1.5 cm in diameter located in the basal ganglion regions
- .The diagnosis is Intra-cranial calcification - (2
-
- The corrected calcium level is = Measured serum Ca level + (40 - (4 .measured serum albumin level) x 0.owes
-
- is the usual normal albumin level, so the corrected Ca level is 1.45 + (40 40 .1.45 + 0.46 = 1.91 mmol/L = (x 0.022.21) + 1.45 = 0.022 x (19
- The cause is high dose of Vitamin D (One Alpha Calcidol ) which was - (3 -used to control hypocalcemia. The hypocalcemia is secondary hypo .parathyroidism which is a part of Middle East Syndrome .(Sanjad Saqqati Syndrome)
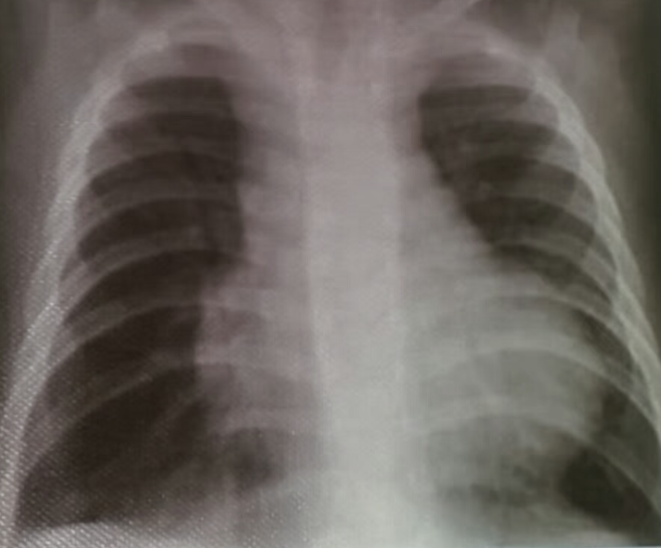
- AP chest film which shows complete opacification of the whole right lung - (1 .with shifted mediastinum and trachea to the left side
- .This indicates pleural effusion (PE) - (2
- After inserting chest tube, pus was coming out. This means that the PE is - (3 .an Empyema
- .The cause of this empyema is most likely a Bacterial Pneumonia - (4
- The age of the patient is 10 years which means that the most likely - (5 .organism is Streptococcus Pneumonae
- .AP plain X-ray of both hands and wrests - (1
- .There are severe osteopenia, rarefaction of bone and wide wrests joints - (2
- Signs of rickets (cupping, fraying and flaring) are evident at the ends of - (3 .the radius and ulna
- AP chest film which shows opacification of the middle and lower zones of - (1 .the left lung. The upper border of the opacity is concave
- .This indicates pleural effusion (PE) - (2
- After inserting chest tube, pus was coming out. This means that the PE is - (3 .an Empyema
- .The cause of this empyema is most likely a Bacterial Pneumonia - (4
- The age of the patient is an 8 years which means that the most likely - (5 .organism is Streptococcus Pneumonae
- AP chest film showing moderately increased heart size. Heart diameter to - (1 .trans-thoracic diameter ratio is 78 %. This is a cardiomegaly
- The cause is Congestive Heart Failure [CHF] secondary to viral - (2 .myocarditis
- AP chest film of the chest which shows a left sided pneumothorax and - (1 .chest tube in place
- There is a thin wall spherical cyst measuring 3 X 4 cm in the upper zoon - (2 .of the right lung. This is called Pneumatocele
- .Pneumatocele can ruptured and leads to Pneumothorax - (3
- Both Pneumatocele and Pneumothorax are complication of Bacterial - (4 Pneumonia caused by Stalhylococcus Aureus, Streptococcus Pneumonae .and Gram Negative Rods such as KleibsellaPneumonae
- AP chest film showing the following; 1)- Laterally located Bilateral - (1 Opacities in both lungs indicating resolving ARDS, 2)- Bilateral hyper-lucent shadows in the Superior Mediastinum which resemble Butter Fly Wings indicating Bilateral Pneumomediastinum, 3)- Rim of air encircling the heart .and indicates Pneumopericardium
- Both of them May be complication of ARDS or secondary the high - (2 .pressure used during Mechanical Ventilation
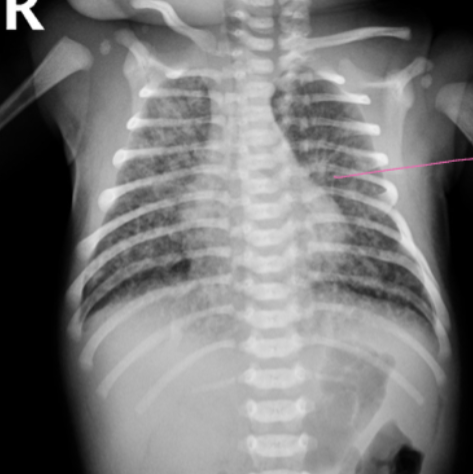
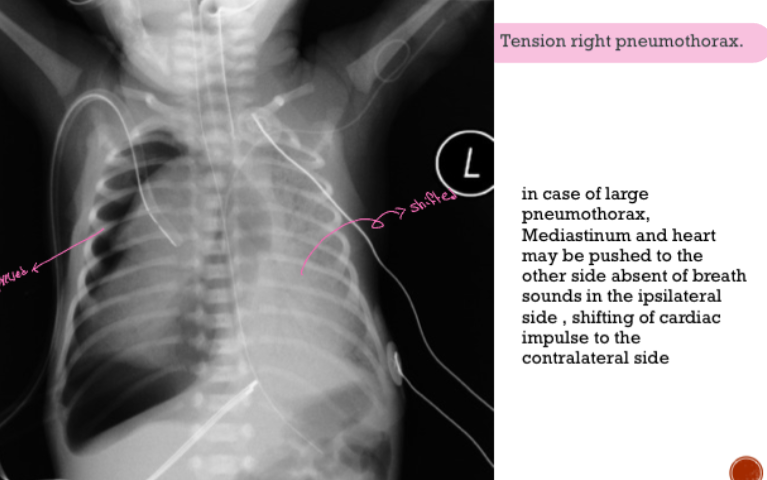
- There is a hyper-lucent area involving the majority of the right hemi-thorax which is devoid of lung tissues. This is separated from the heart with a very well demarcated opacity. The hyper-lucent area is a pneumothorax and the well demarcated opacity is the severely compressed right lung from the .pneumothorax
- .The diagnosis is a Right Sided Tension Pneumothorax -
- .This is a killer if not drained immediately -
- The physical examination of the chest will not show the typical signs seen in ,adult, however, limitation of movement and plugging of the right hemithorax displaced heart sounds more laterally and absent air entry over the right side .can be found
- The Bed Side Test which can be used for the diagnosis is the -
-
Transillumination of both hemi-thorax using a strong beam of light. The area of the transillumination over the side of the pneumothorax is far larger and wider .than the normal side
-
The treatment must be immediate without waiting for chest X-ray - confirmation. The collected air is evacuated by a butterfly needle connected to a 3 stop-cock connector which is attached to a 20 or 50 ml syringe. The -needle is inserted perpendicularly in the 2d inter-costal space (ICS) at the mid clavicular line until a gush of air is seen. The air is then aspirated by the .syringe then pushed to the outside. More than 2 aspirations may be needed
-
You may aspirate 200 ml in severe cases
-
.The needle evacuation is followed by chest tube insertion -
-
It is known for bronchiolitis to be complicated by pneumothorax because of - air-trapping and hyper-inflation of the lung secondary to inadequate deflation .from bronchioles narrowing by inflammation, edema and bronchospasm
-
The CBC and differential counts show severe leucocytosis and - (1 neutrophelia. The platelets count is high. Both the ESR and the CRP are markedly high. All of the above including high platelets are called Acute .Phase Reactant and found during severe infection such as Pyelonephritis
-
The radiological test shown is called Micturating Cysto-urethrogram - (2 .or voiding cysto-urethrogram (VCUG) (MCUG)
-
There is reflux of the dye up to the collecting system with cupping of calyces - and tortuosity of the ureter in the right side (Vesico-urethric Reflux [VUR] grade .V)). The left ureter is less severely affected
-
The patient is slightly hypertensive which means there is residual damage - .from recurrent UTI
-
For that reason, she needs further investigation such as Renal U/S looking for hydronephrosis and assessing the echogenicity of the kidneys, DTPA for functional assessment of renal function and DMSA to look for renal scar from .previous UTIs
-
Prostaglandin
-
Surgery
-
IGA
-
Tricuspid Atresia

- Name the test?
- Voiding cystourethrogram (VCUG)
- List Findings?
- posterior urethral valve
- dilated ureters
- tortious ureters
- dilated uretric pelvic bilaterally (hydronephrosis)
- Diagnosis?
- VesicoUretral Reflux (VUR)
 Central cyanosis, baby crying, bloody face, blue due to TGA. Z
General Note: Pay attention: Differentiate between this and the Egg shape in TGA
Central cyanosis, baby crying, bloody face, blue due to TGA. Z
General Note: Pay attention: Differentiate between this and the Egg shape in TGA
X-Ray Description:
- Cardiomegaly
- Enlargement of the right atrium and right ventricle is most apparent.
- Prominent pulmonary vascular markings.
- Differential Diagnosis (DDX): AVSD, ASD, VSD
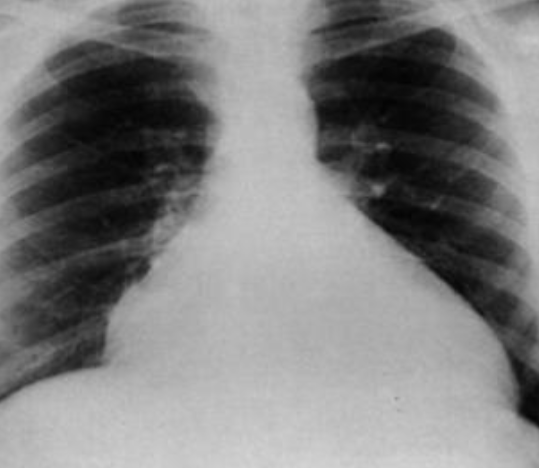
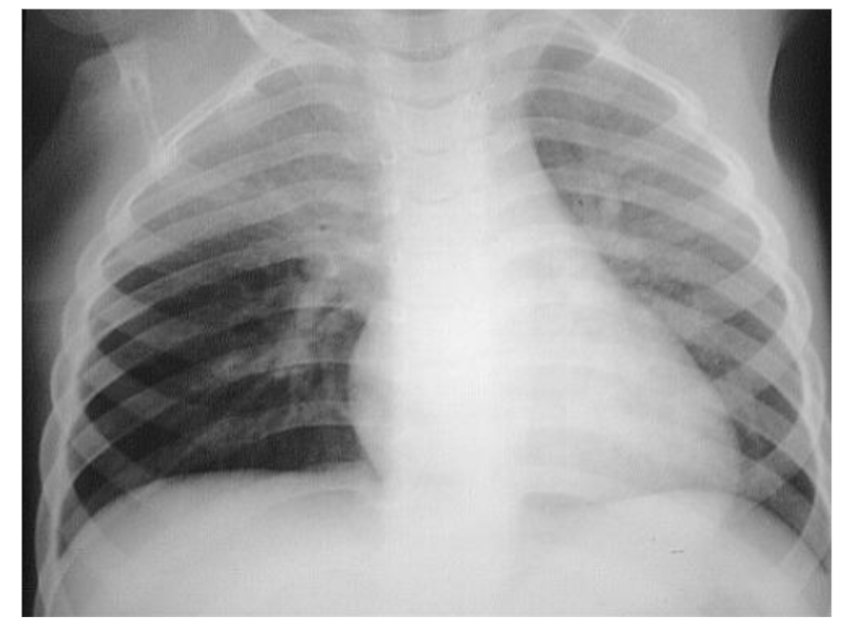
 X-Ray with Consolidation:
X-Ray with Consolidation:
- What is the diagnosis? Pneumonia
- What is the causative organism? Streptococcus Pneumonia
 X-Ray with Double Bubble Sign:
X-Ray with Double Bubble Sign:
- What is the diagnosis? Duodenal Atresia
- What is the curative management? Deudenostomy
 Heart Failure:
Heart Failure:
- Diagnosis: Heart failure (nonspecific)

- Description: cardiomegaly, increase pulmonary vascular markings (plethoric lung fields)
- DDx: VSD, AVSD

- Description: marked cardiomegaly extends from wall to wall (Box Shape)
- Diagnosis: Ebstein Anomaly

- Boot-shaped, no vascularity in lung parenchyma with cyanosis, TOF Z
- Description: Boot shape heart with upward cardiac apex due to Right ventricular hypertrophy and concave pulmonary artery segment and decrease pulmonary vascular marking at peripheral lung field. Z
- Describe 2 abnormalities seen in the X-Ray?
- Boat-shaped heart
- Narrow mediastinum
- What is the likely diagnosis? Tetralogy of Fallot’s (TOF)
- What is the name of this maneuver? *
- Knee chest position (Squat maneuver)
- What is the purpose of this maneuver? *
- To treat episodes of TOF

- To treat episodes of TOF
- Describe 2 abnormalities seen in the X-Ray?
 Knee Chest Position:
Knee Chest Position:
- Description: Knee chest position (Squatting position) to treat the episodes of TOF

- Senior: 3-month-old with heart failure, cyanotic, and cardiac murmur
- Description: small heart, pulmonary edema
Pulmonary Venous Stenosis
What is observed in the chest X-ray? Heart failure without signs of cardiomegaly.
What is the likely diagnosis? Pulmonary Venous Stenosis.
 Transposition of Great Arteries:
Transposition of Great Arteries:
- Description: Egg on string Transposition of Great Arteries Z
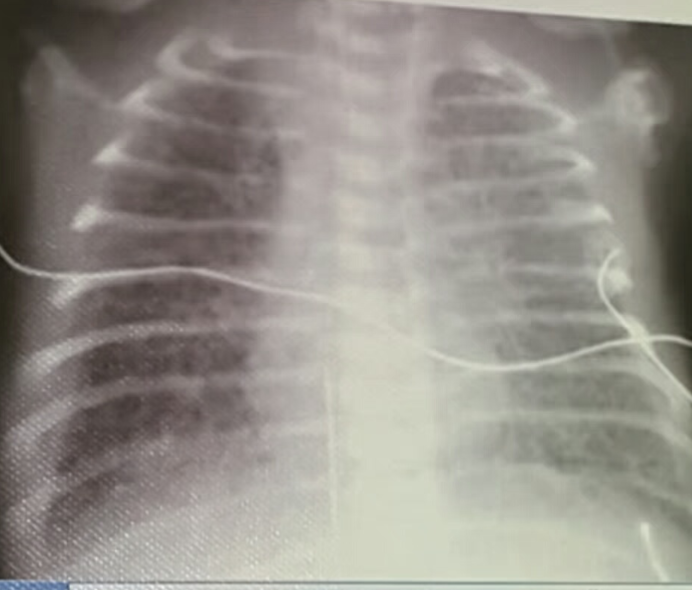
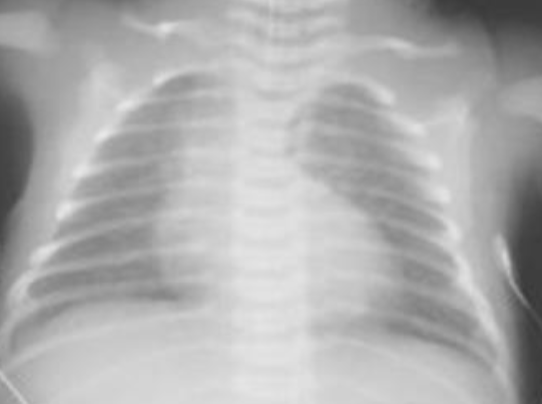
 MECONIUM ASPIRATION:
MECONIUM ASPIRATION:
- Hyperinflation, Consolidation, Patchy infiltrates
- If severe, air leak and pneumomediastinum may occur
NECROTIZING ENTEROCOLITIS:
- (A) Dilated loops, Thickened bowel walls
- (B) Pneumatosis intestinalis (air in intestinal walls) because the distention
- Pneumoperitoneum
- Portal gas (present in the portal venous system)
- Pneumoperitoneum is an emergency requiring surgical intervention
- Portal gas represents air and is considered to be a poor prognostic sign.

Case Study: Child Abuse
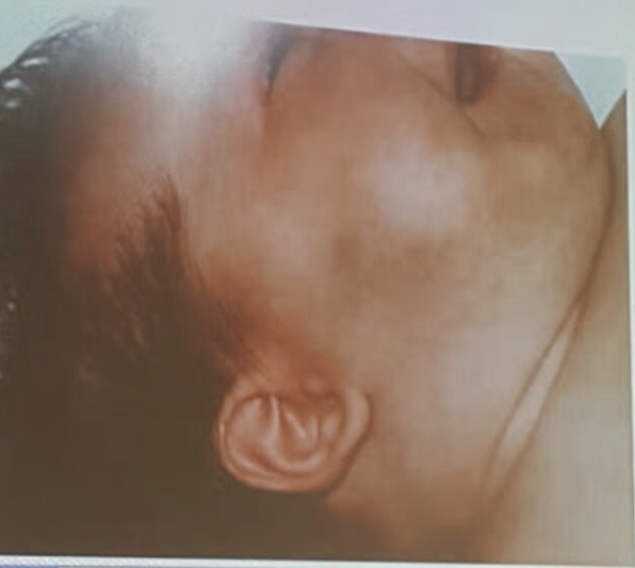
- Bruises on cheek
- Fracture Ribs → child Abuse
Left to Right Shunt (ASD, VSD)
Failure to thrive, recurrent chest infections, and a cardiac murmur.
What is the likely diagnosis based on the chest X-ray? Left to Right Shunt, possibly ASD or VSD, leading to congestive lung.

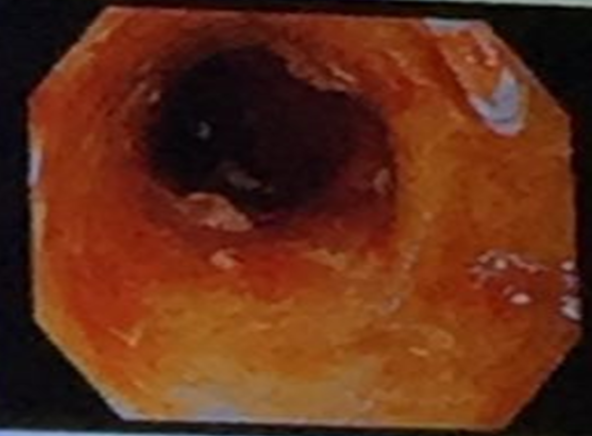
Crohn’s Disease
What is observed in the X-ray? Cobblestone appearance. What is the likely diagnosis? Crohn’s disease.

Cardiomegaly (AVSD, ASD, VSD)
What is observed in the X-ray? Cardiomegaly with enlargement of the right atrium and right ventricle, and prominent pulmonary vascular markings.
What are the possible diagnoses? AVSD, ASD, and VSD.

Diagnosis: Ulcerative Colitis
- X-ray shows: Lead pipe appearance
Case
Fever and bloody diarrhea Diagnosis ? Ulcerative colitis
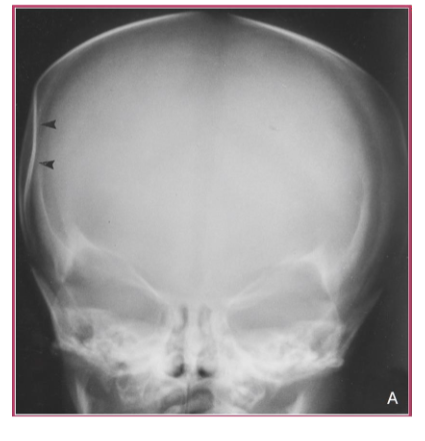
Diagnosis: Depressed Skull Fracture Z
- Conventional skull radiograph showing the typical depressed, ‘‘ping-pong’’ fracture of the newborn.
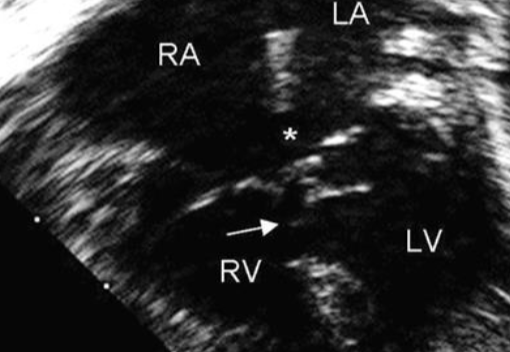
Investigation and likely diagnosis
- Echocardiography.
- Complete Atrioventricular Septal

4-month-old infant with heart failure
- X-ray show? A snowman appearance (figure of 8 heart).
- Diagnosis? Total Anomalous Pulmonary Venous connection.

X-ray finding
- Thick abdominal wall
- Dilated bowel loops
- Abnormal gas pattern
- Diagnosis? Necrotizing enterocolitis
- What is the most immediate action (therapy) you will provide? Broad-spectrum antibiotics

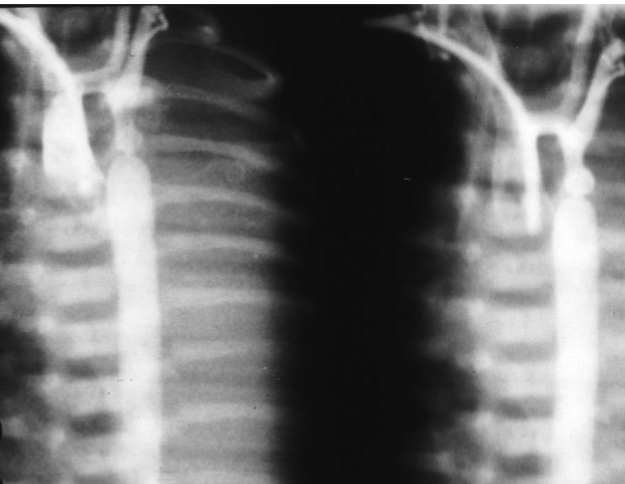
Croup
- Sign? Steeple sign.
- Diagnosis? Croup.
Case
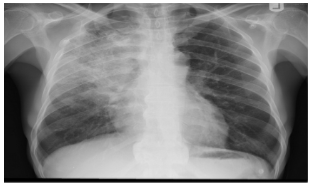
Diagnosis ? Lobar pneumonia Most common cause ? Streptococcus pneumoniae

Case
Diagnosis? Pneumothorax
Case
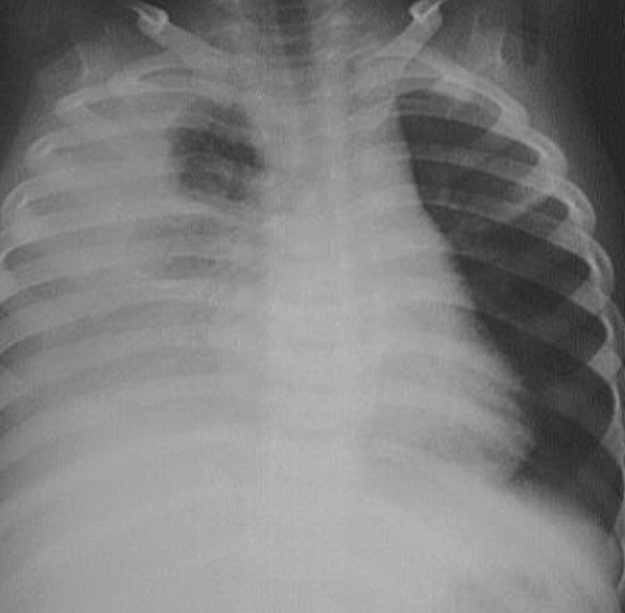
Diagnosis ? Pleural effusion

Case
9 month old infant with poor weight gain, recurrent chest infection and cardiac murmur. WRITE 2 ABNORMALITES IN THE X-RAY? Cardiomegaly. increase pulmonary vascular marking differential diagnosis? VSD, ASD, PDA
Case
write the type of the investigation and the likely diagnosis? Aortic angiography by cardiac catheterization.
Coarctationof aorta
Case
Newborn with jaundice, microcephaly, IUGR and hearing loss, the mother is rubella immune Purple skin lesion and petechiae with hepatosplenomegaly
what is the investigation ? Brain CT Diagnosis ? Toxoplasmosis