Acute Abdomen
The Dangerous Miss: Recognizing Acute Mesenteric Ischemia
80% of acute mesenteric ischemia cases result in mortality because of missed diagnosis. Here’s how to recognize the signs.
Mesenteric Ischemia
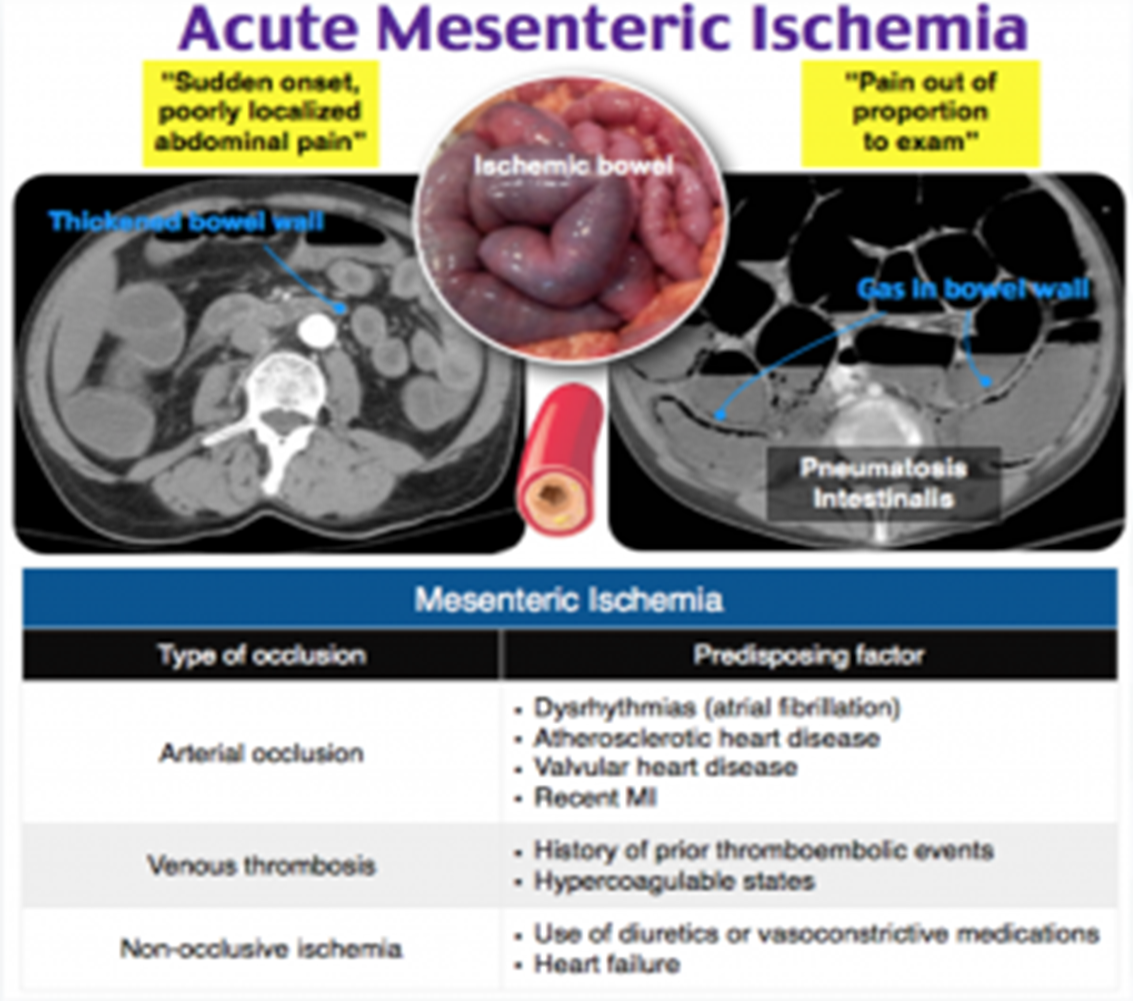
Traditionally, mesenteric ischaemia presents with a generalised abdominal pain, out of proportion to the clinical findings, although it can often be more variable or subtle than this. The patient will typically complain of a diffuse and constant pain, with associated nausea and vomiting present in around 75% of cases On examination, the abdomen is often unremarkable and the patient may find it difficult to localise the pain. However, remember late stage bowel ischaemia and necrosis can present as bowel perforation. Importantly, take note of any potential embolic sources, such as AF, heart murmurs, or signs of previous valvular replacement surgery

Small Bowel
Mesenteric ischemia
-
Arterial or Venous
-
Acute or Chronic
-
Symptoms:
- Non-specific
- Severe abdominal pain out of proportion to the degree of abd. tenderness
- Diarrhoea (watery, bloody)
- Acute: Sudden abdominal pain, passage of altered blood, shock.
- Chronic: Abdominal angina, “food-fear”, weight loss or diarrhoea.
-
Signs:
- Abdominal tenderness
- Guarding
- Rigidity
- Symptoms are out of proportion to signs
Predisposing factors:
- Thrombophilia
- Hyper-viscosity
- Gut hypo-perfusion
- Shock (hypovolemic- cardiogenic-septic)
- Cardiac arrhythmia
Causes:
- Arterial:
- Arterial embolus : (most common-50%; heart; usually lodge distal to origin of the middle colic
- Recent MI- Atrial fib
- Polycythemia- SCD- DIC
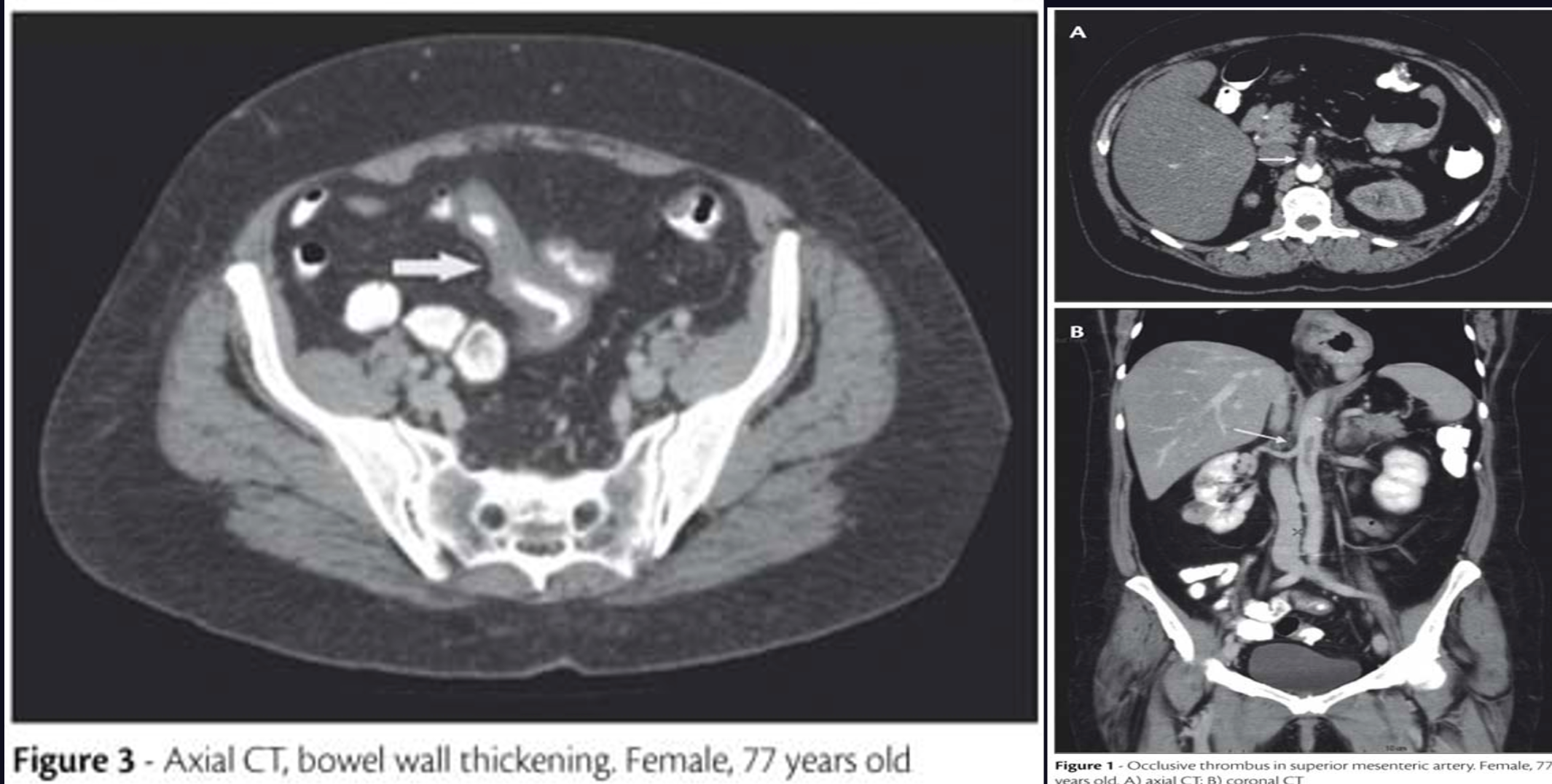
- Arterial thrombosis
- Venous thrombosis : (5-15%) and 95% SMV
- Vasospasm (non-occlusive mesenteric ischemia – NOMI):
- usually in critically-ill pt.
- Receiving vasopressors.
Investigations:
- Labs:
- High WBC- High lactic acid- high amylase
- ABG (metabolic acidosis)
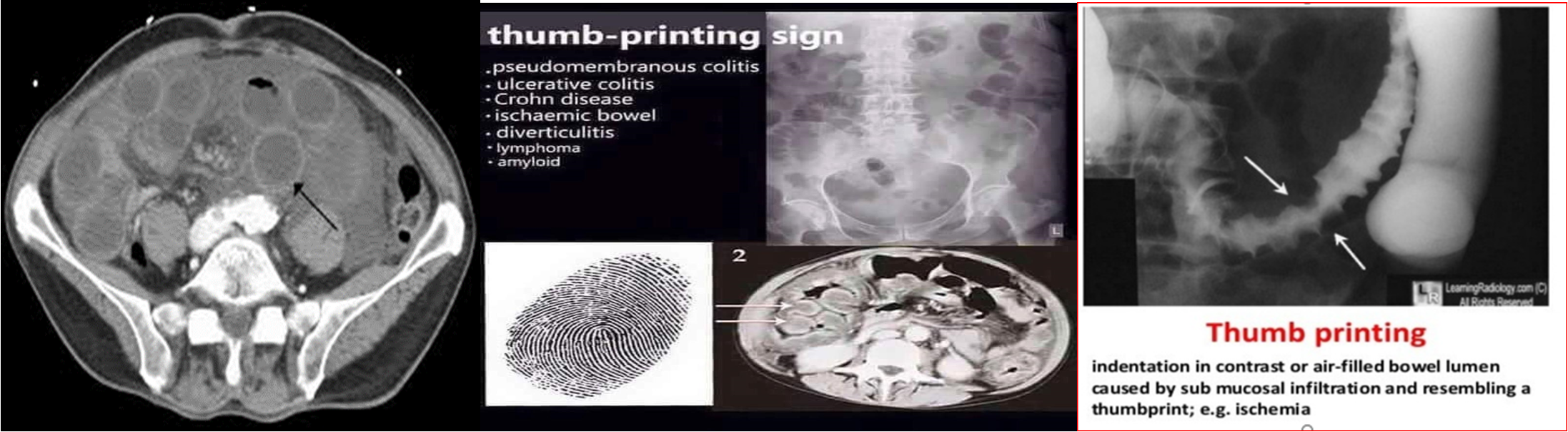
- AXR
- Thickened, dilated gas-filled bowel
- Gas in bowel wall
- CT angiography
- Exclude other pathology
- Assess mesenteric vasculature, intestine & its mesentery
- Test of choice for acute mesenteric venous thrombosis
Treatment:
- Resuscitation,
- Golden hours
- Anticoagulation, & thrombolysis
- Surgical option:
- Bowel Resection,
- Embolectomy, thrombectomy
- Vascular bypass or Endarterectomy (If stable patient)
Surgical indications:
- signs of peritonitis :
- Necrotic : segmental resection
- Questionable viability: second look