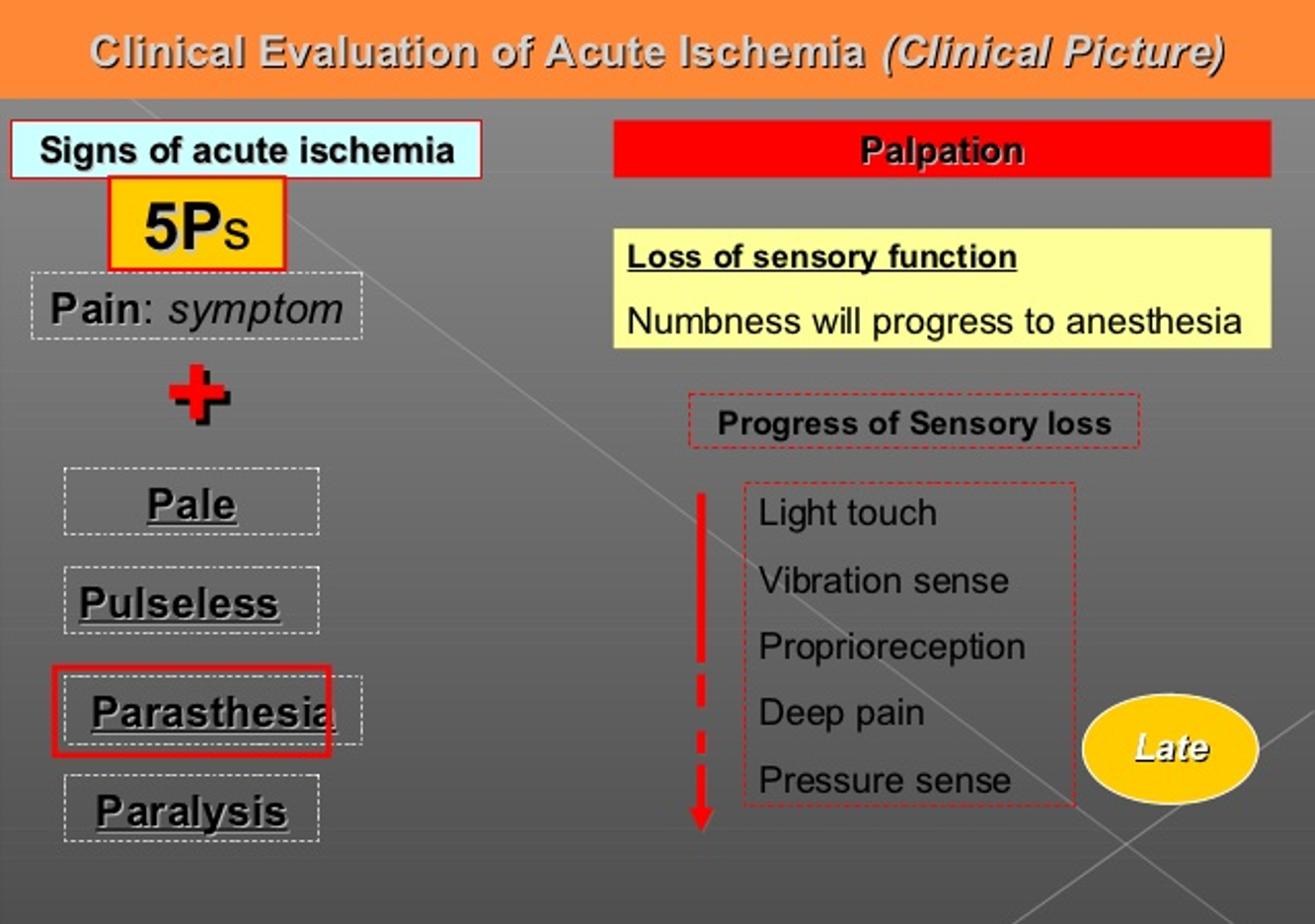
 Early -⇒ Late
light touch ⇒ vibration ⇒ Proprioreception ⇒ Deep pain ⇒ Pressure sense
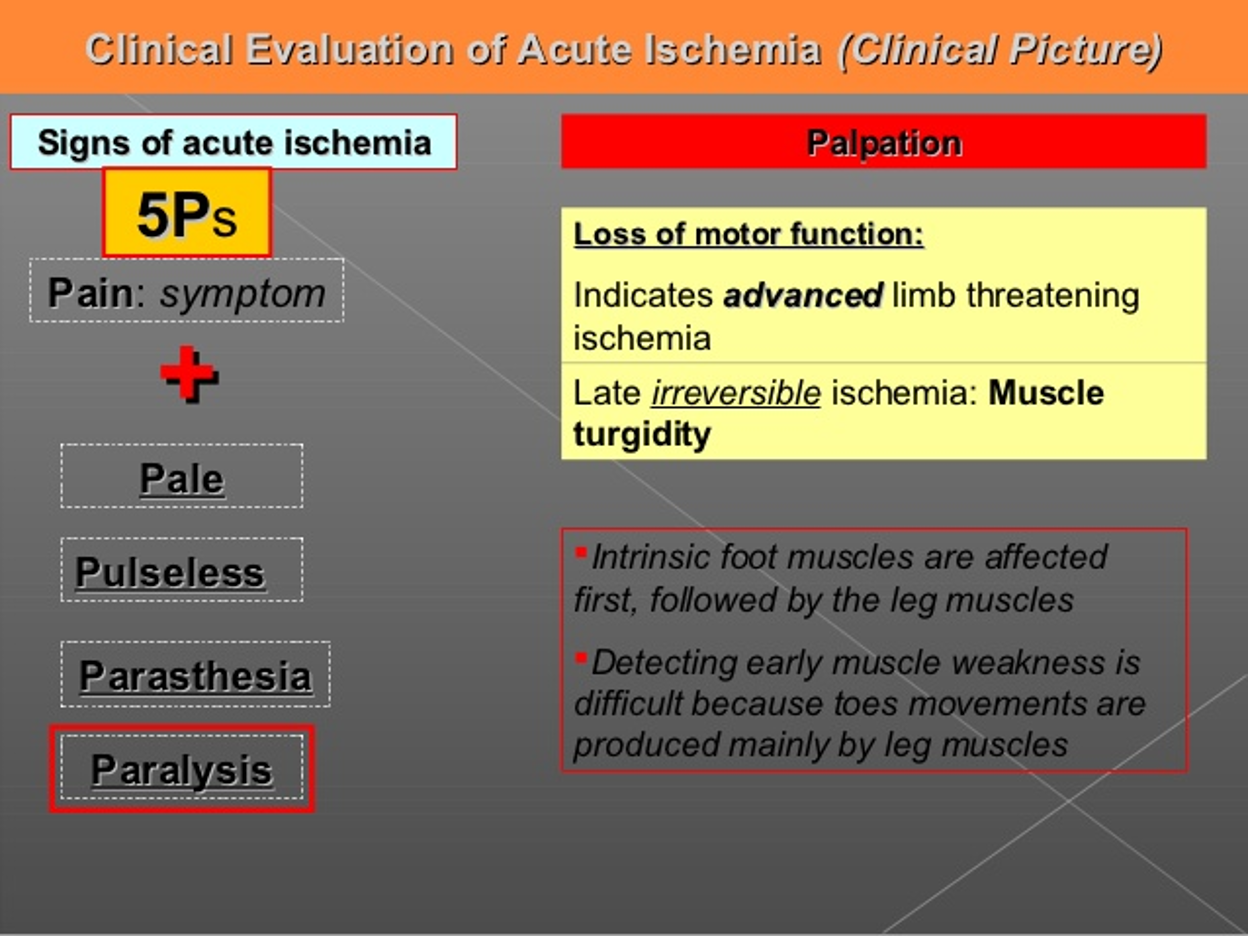
Early -⇒ Late
light touch ⇒ vibration ⇒ Proprioreception ⇒ Deep pain ⇒ Pressure sense
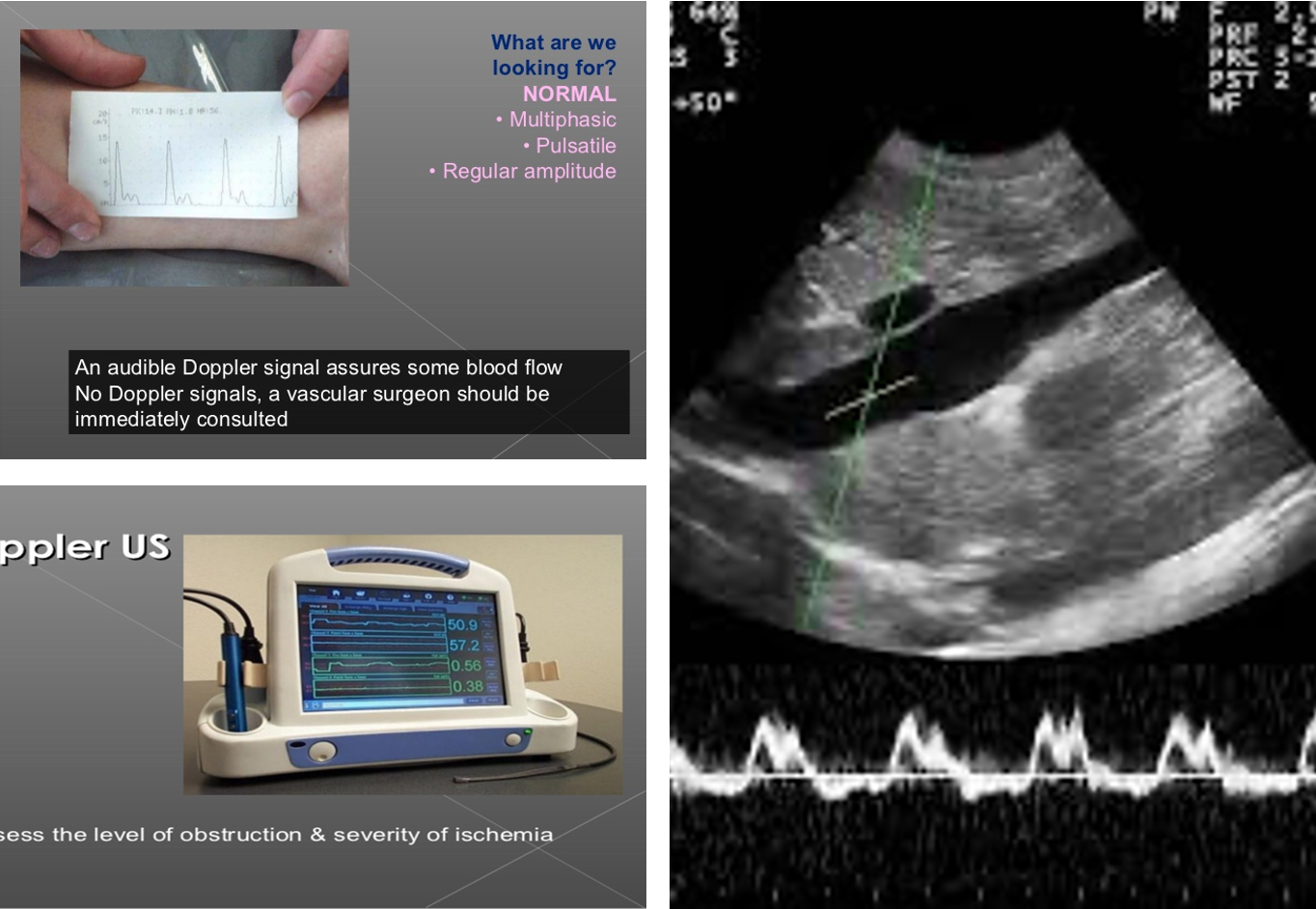
Doppler Vs Dopplux
Multiphasic normal one -
duplex waves + picture
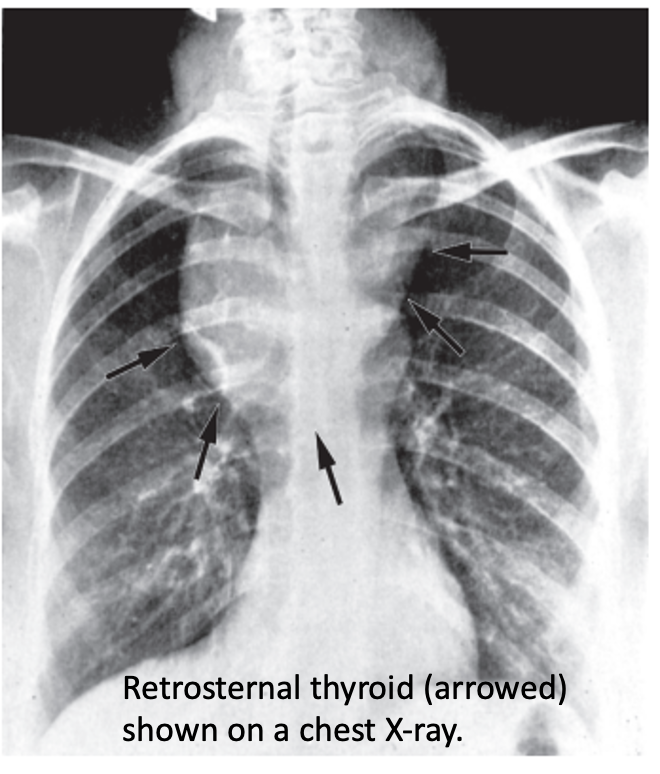
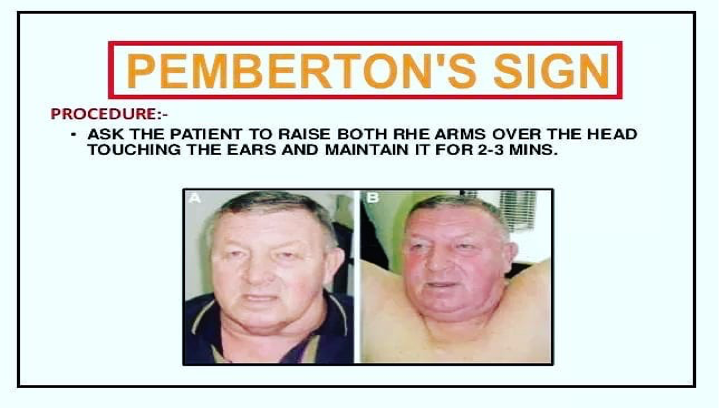 Pemberton’s sign is used to evaluate venous obstruction in patients with goiters. The sign is positive when bilateral arm elevation causes facial plethora. It has been attributed to a “cork effect” resulting from the thyroid obstructing the thoracic inlet, thereby increasing pressure on the venous system.
Pemberton’s sign is used to evaluate venous obstruction in patients with goiters. The sign is positive when bilateral arm elevation causes facial plethora. It has been attributed to a “cork effect” resulting from the thyroid obstructing the thoracic inlet, thereby increasing pressure on the venous system.
Epigastric hernia
- Protrusion through a defect in linea alba, Firm midline lump.
- Often contains preperitoneal fat or peritoneal sac with omentum
- Open surgical repair by non-absorbable suture or mesh
- Laparoscopic repair- if large

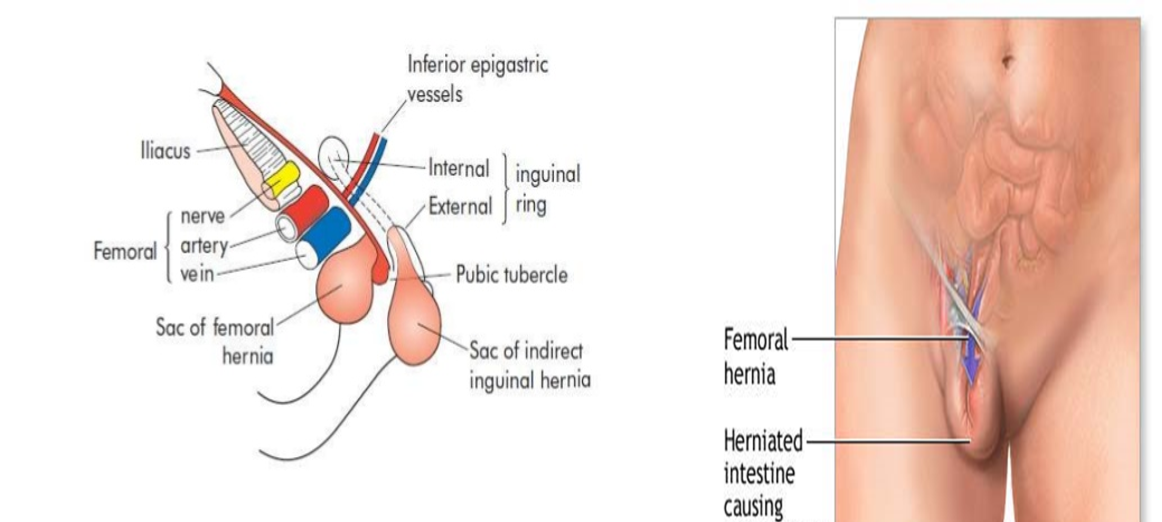
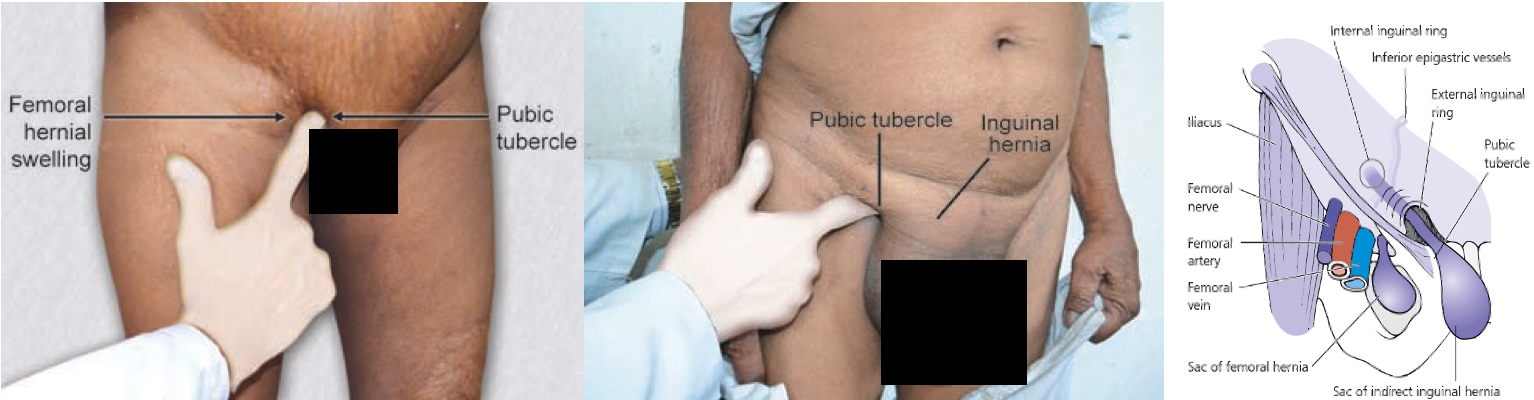
Femoral hernia
- Projects through femoral ring and passes down the femoral canal (1.25 cm)
- Appears, to lie in front of inguinal ligament
Clinical features of Femoral hernia
- Groin swelling - often small
- Groin pain on exercise
- Often irreducible due to its curved course
- Sometimes difficult to distinguish with IH
- Examination: Put a finger tip over pubic tubercle (How to find it?) IH- above & medial FH- below & lateral
- Obstruction, strangulation rate high (40%)
Differential diagnosis- Femoral hernia
- Lymphadenopathy : Cloquet’s node
- Saphenous varix- thrill on cough, disappears on lying down
- Inguinal hernia
- Ectopic testis
- Psoas abscess
- Femoral aneurysm
- Soft tissue neoplasms as lipoma
more desposed to strangluation

Incisional hernia
- Hernia through poorly healed abdominal incisions
- More common with midline vertical incisions
Predisposing factors:
- Poor surgical technique: Layered closure, absorbable suture, suturing under tension, drain tubes are brought out through the main wound
- Preoperative straining factors: Chronic cough, chronic constipation and urinary obstruction.
- Postoperative complications: Abdominal distension, cough, respiratory distress due to pneumonia or lung collapse, and postoperative wound infection.
- General factors: Age (elderly patients), malnutrition, hypoproteinemia, jaundice, malignancy, diabetes, chronic renal failure, steroid or immunosuppressive therapy and alcoholism.
Gastric Adenocarcenoma:
- 95% of all malignant gastric neoplasms
- Twice as common in men as it is in women,.
- Increases with age, peaking in the seventh decade.
- More at gastric cardia
Risk factors:
- Nutritional
- Environmental
- Social
- Medical
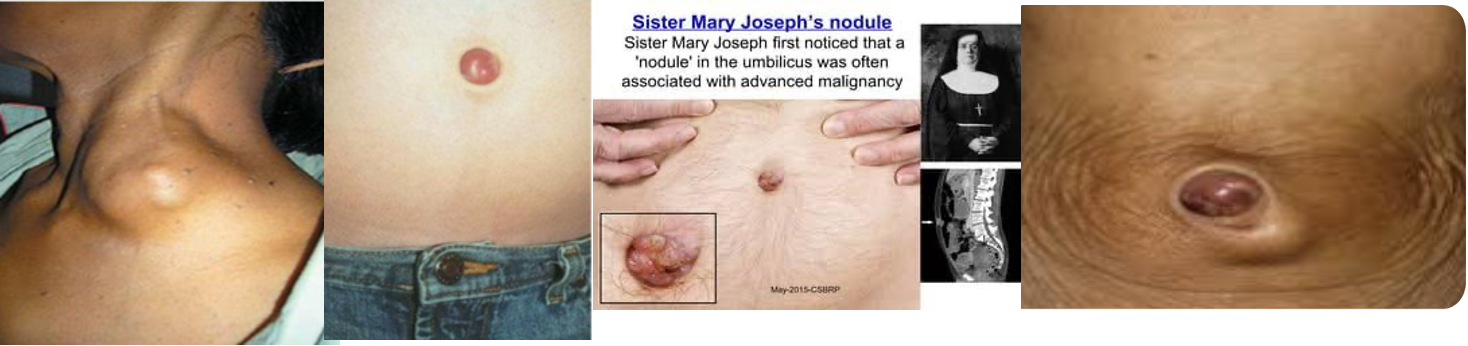
- left supraclavicular lymph virchow sign
- , 3, 4 sister mary joseph nodules
S/S
-
Significant GI bleeding is rare
-
15% of patients may develop hematemesis,
-
40% of patients are anemic.
-
Physical signs develop late & associated with locally advanced or metastatic disease.
-
Palpable abdominal mass,
-
Palpable supraclavicular (Virchow’s)
-
Periumbilical (Sister Mary Joseph’s) lymph node,
-
Peritoneal metastasis palpable by PR (Blummer’s shelf),
-
Palpable ovarian mass (Krukenberg’s tumor).
Plain x-ray- CXR, AXR, tomograms
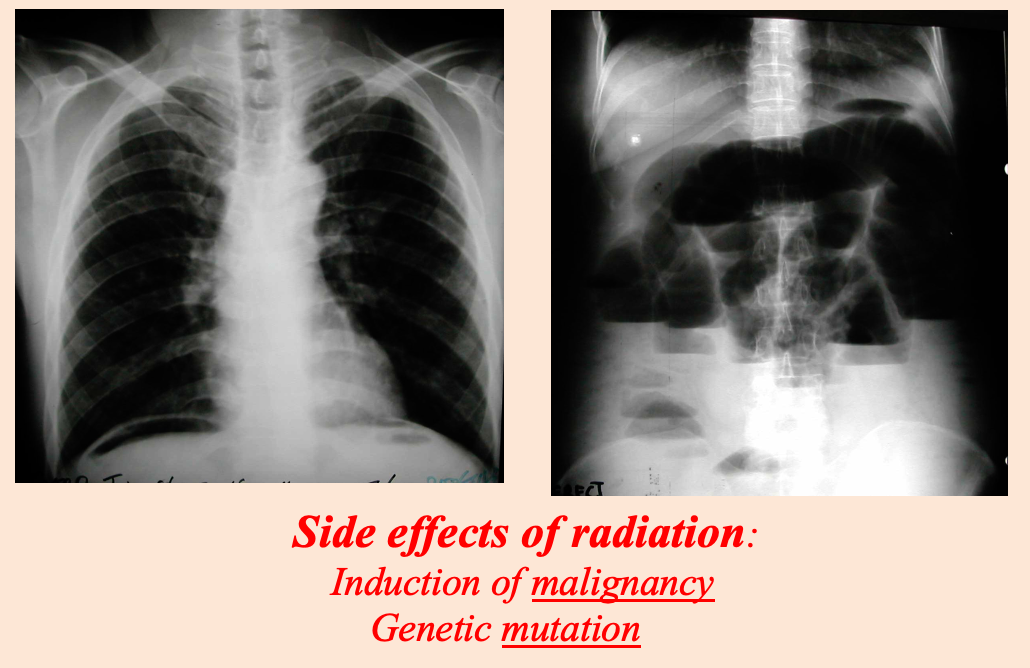 Modality: plain x-ray
Findings: air under diaphram / multiple air fluid levels
Differentials: perforation / obstruction
Modality: plain x-ray
Findings: air under diaphram / multiple air fluid levels
Differentials: perforation / obstruction
Side effects of radiation:
- Induction of malignancy
- Genetic mutation
Subcutanous emphysema

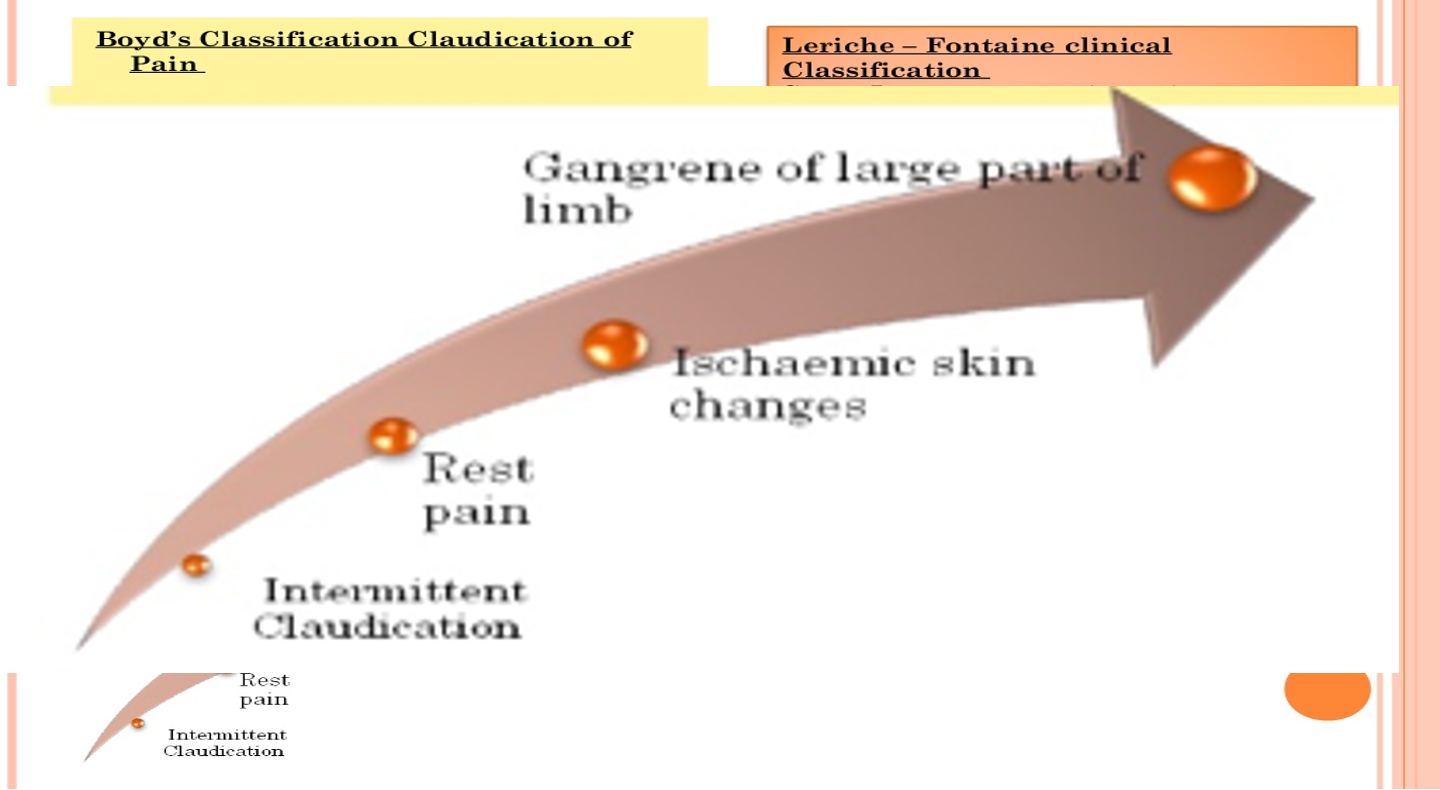 Intermittent claudications ⇒ Rest pain ⇒ Ischemic skin changes ⇒ gangrene Large part of limb
Intermittent claudications ⇒ Rest pain ⇒ Ischemic skin changes ⇒ gangrene Large part of limb
Deep Vein Thrombosis:
-
- Post-operative.
-
- Immobility due to other illness.
-
- Leg pain.
-
- Leg swelling.
Superficial thrombophlebitis:
- Inflammation & thrombosis of previously normal superficial vein.
- Pain, redness and cord like vein
antibiotic enough

Venous ulcer:
- Previous DVT , Varicose Veins
- Above medial malleolus (70%)

Infection- lymphangitis
Inspection:
- Red streaks and swelling of the limb
- Site of primary infection may be visible
- Spreading
Palpation:
- Warm, tender, pitting oedema
- Palpable and tender draining lymph node

Lymphedema
- Primary lymphedema: Congenital, due to poorly developed lymphatics
- Secondary: Infective (Filariasis) or neoplastic (secondary deposits)

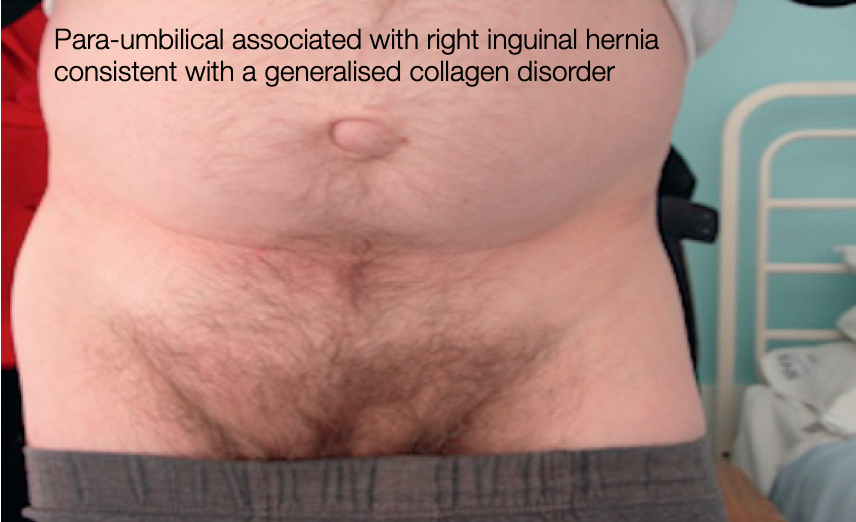
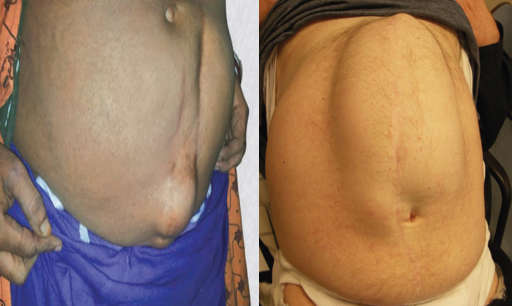
 1- abcess 2- periumbilical hernia 3- inisional hernia
1- abcess 2- periumbilical hernia 3- inisional hernia
 ascites / caput medusa
ascites / caput medusa
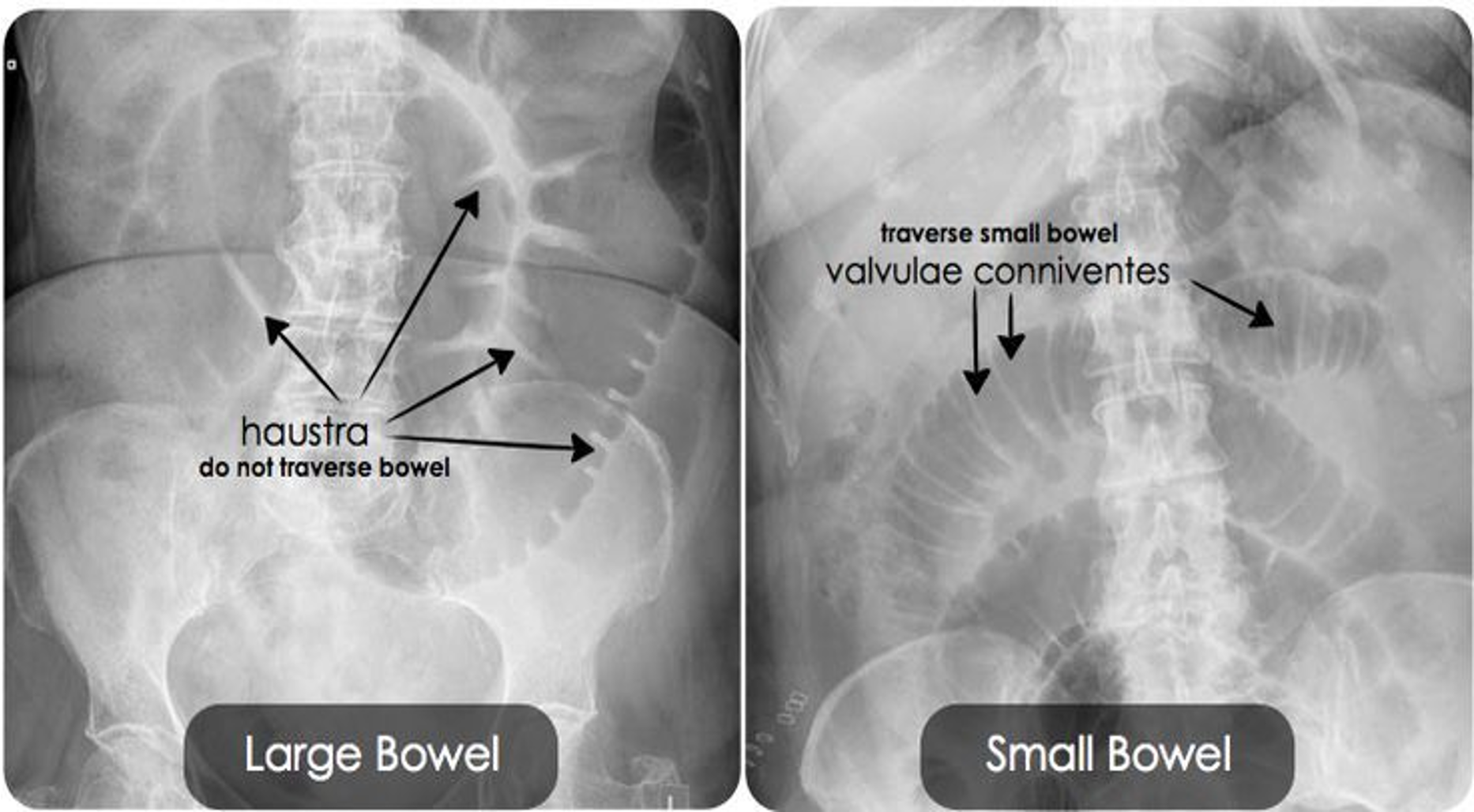
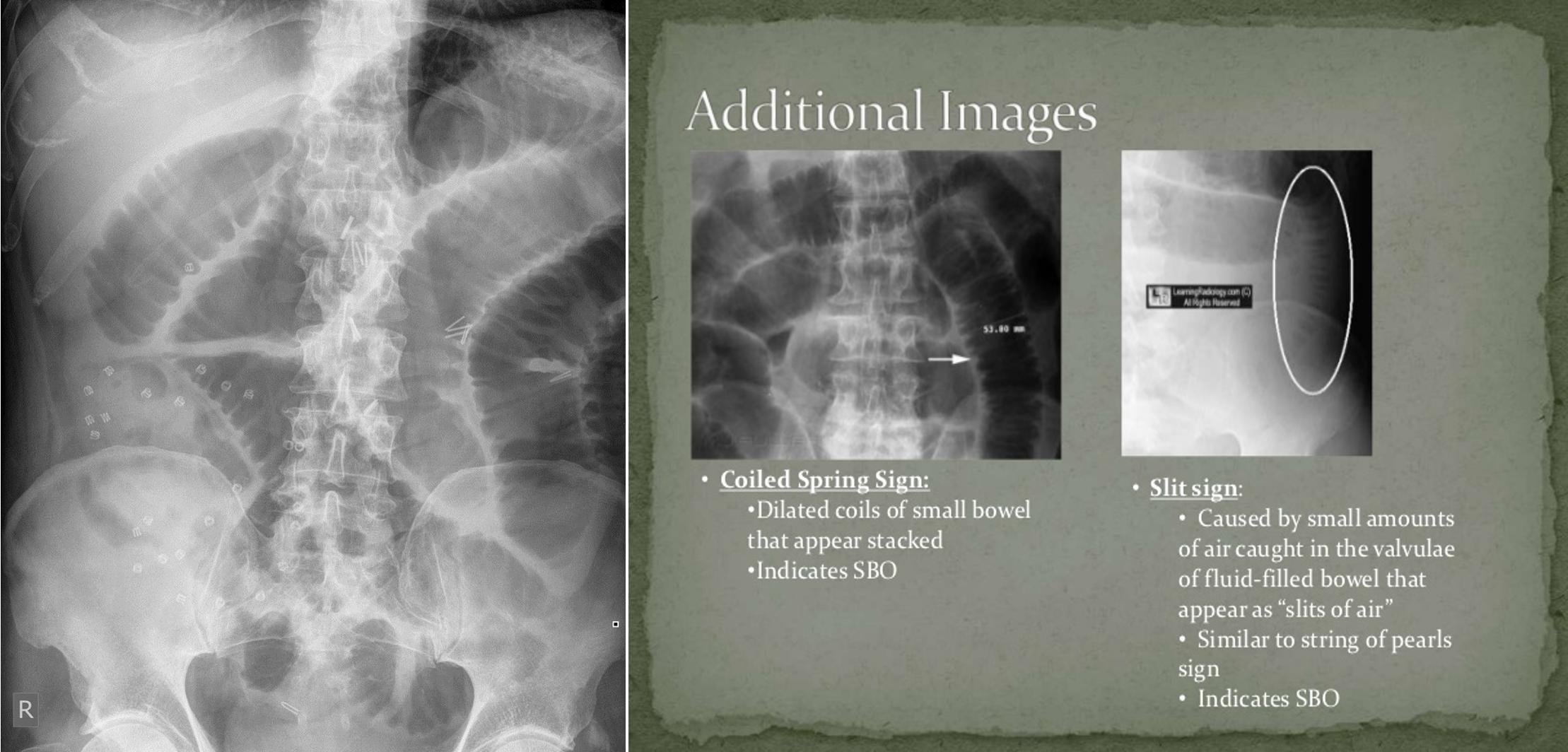
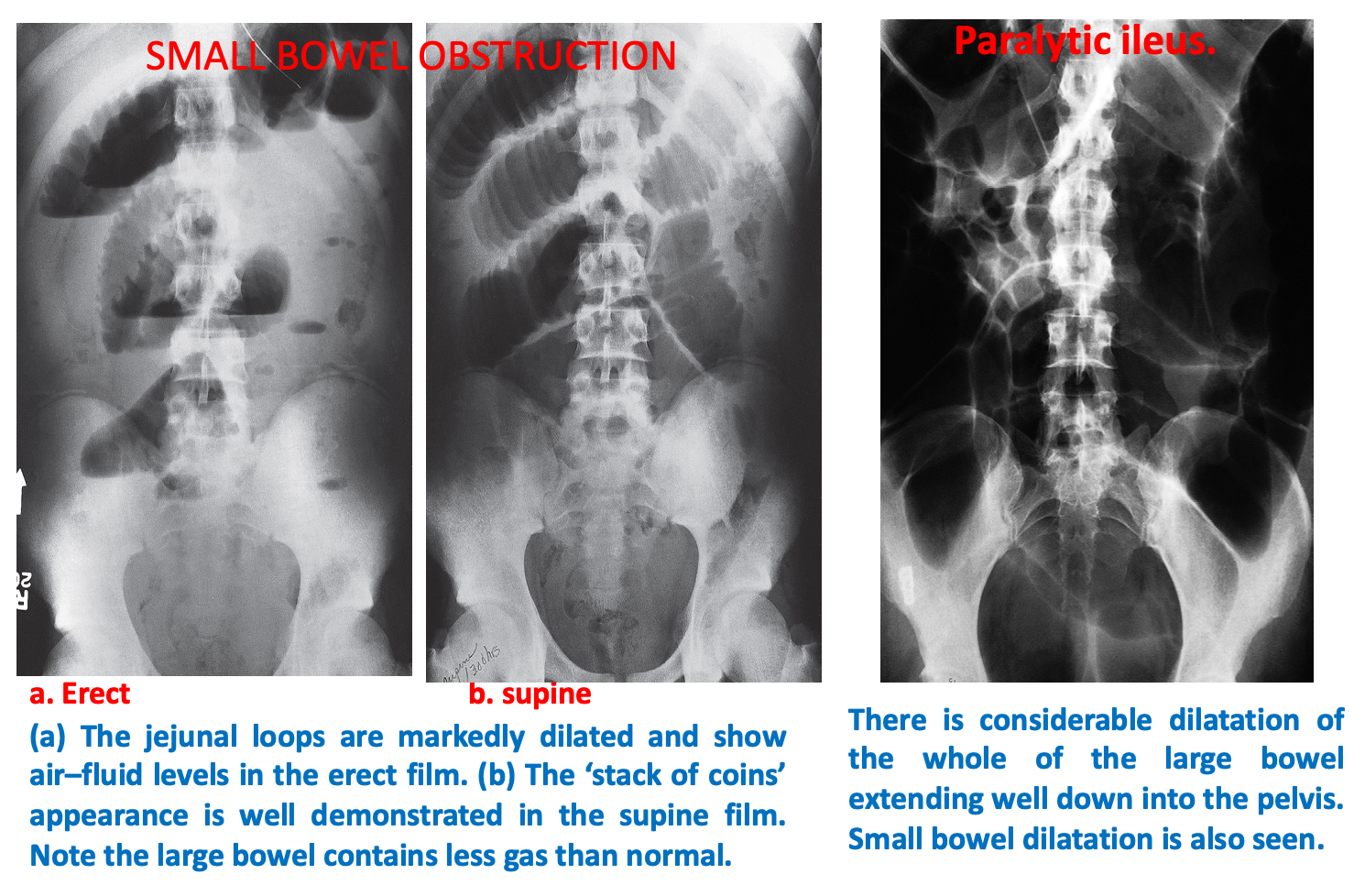
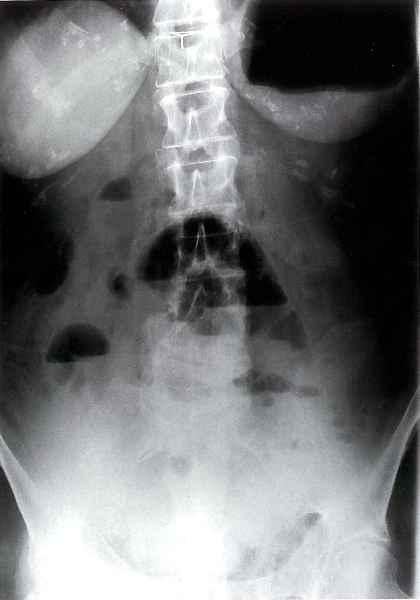 Mechanical small bowel obstruction-X-ray abdomen (erect)
Multiple air-fluid levels are visible in the mid-abdomen. The opaque appearance of the pelvis is due to fluid-filled loops of small bowel. There is a paucity of gas in the colon, and an air-fluid level is present in the dilated stomach.
Mechanical small bowel obstruction-X-ray abdomen (erect)
Multiple air-fluid levels are visible in the mid-abdomen. The opaque appearance of the pelvis is due to fluid-filled loops of small bowel. There is a paucity of gas in the colon, and an air-fluid level is present in the dilated stomach.