Management of patients with multiple trauma
Dr. Ahmed Khan
Hospital care
ATLS approach (Advanced Trauma Life Support)
-
Primary survey: initial assessment & management
- Treat the greatest threat to life
- Immediate intervention as the threat to life identified
- Detailed history not essential
- Re-evaluation of initial management
-
Secondary survey: a head to toe evaluation
Primary survey- “a team approach”
- Multiple providers
- Simultaneous diagnosis & treatment
- Reduces the time to assess & stabilize
- Team is organized before patient arrival.
- Leadership & unity of command-essential
Primary survey- “one clinician”
Do not perform subsequent steps in the primary survey until after addressing life-threatening conditions in the earlier steps.
Primary survey
A B C D E
- Airway & cervical spine protection
- Breathing & ventilation
- Circulation with control of external bleeding
- Disability (neurologic assessment)
- Exposure & Environmental control- undress, prevent hypothermia
Adjuncts to Primary Survey & resuscitation
- Oxygen
- Pulse oximetry
- BP monitoring
- ECG monitoring
- NG tube, urinary catheter (urine sample)
- Ventilatory rate
- ABG levels
- X-ray- chest & pelvis (AP)
- FAST, ? DPL
Secondary Survey
-
Only after completion of primary survey - Once all life threatening injuries dealt & - Normalization of vital signs
-
Secondary Survey:
- AMPLE history (Allergies, Medication, Past/Pregnacy, Last meal, Events of trauma)
- Examination (Head to toe)
- Continuous reassessment of vital signs
- Additional laboratory/ radiological tests.
- Additional tubes, lines and monitoring devices
- Priorities and plan definitive management of all injuries
Types of injuries
-
- Tension pneumothorax.
- Open pneumothorax (open chest wound).
- Flail chest with underlying pulmonary contusion.
- Massive Hemothorax.
other medical emergencies
Epidemiology
- Most common cause of death (ages 1 and 44 years).
- Affects a disproportionate number of young people
- Burden to society- lost productivity, premature death, & disability.
- A major public health issue.
RTA
Arab News
- 20 deaths daily on the Kingdom’s roads.
- Last year- 707 amputations due to RTA.
- Accidents increased by 78% in the KSA recently
- Affecting mostly young (18 and 22 years)
- Around 30% of injured- permanently disabled.
- The state spent SR21 billion treating such patients
Mobile phones leading cause of road deaths

Types of trauma
-
Blunt trauma: an impact from blunt object.
-
Penetrating trauma: an sharp object piercing the body. Assessment & diagnosis: blunt injuries more difficult than of penetrating injuries
- Multi-trauma: injury affecting simultaneously different organ and body system
Causes of trauma
- RTA or MVA
- Pedestrian trauma
- Fall from height
- Assault
- Firearm injuries
- Knife
- Industrial accidents
- Natural disasters
- Explosions
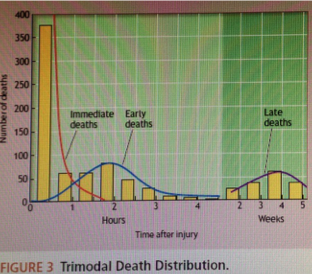
Trimodal death in trauma
-
Immediate: Deaths within seconds or minutes after injury. 50% deaths due to injury to the aorta, heart, brainstem, or spinal cord or by acute respiratory distress. // prevention
-
Early: Death within hours of injury- approx. 30% of deaths. Half die of hemorrhage, the other half due to CNS injury. Can be saved by appropriate treatment- golden hour.
-
Late: Deaths in days to weeks.
- Infection & multi organ failure.
- Care provided earlier impacts the outcome.
 ALTS Manual
ALTS Manual
Improvement in mortality
- Early deaths:
- Prevention and control program
- Legislation & behavior modification
- Later deaths:
- Trauma centers providing better care.
- Better understanding of pathophysiology of multiple organ failure and brain injury
Pre-hospital care
-
Deliver to hospital as rapidly as possible- scoop & run
-
Only Critical interventions at the scene:
-
Airway, hard collar, spine board, control external bleeding.
-
Infusion on way to the hospital
Triage (sort out)
Definition: To Prioritize victims (Multiple) based on – — severity of injury, — likelihood of survival, & — urgency of care.
Goals:
- Identify high-risk injured patients who would benefit from the resources available.
- Limit the excessive shifting of non-severely injured patients so that the trauma center is not over crowded.
Special attention!
- Children: anatomic/ physiologic variations
- Pregnant: anatomic/ physiologic variations, 2 patients!
- Elderly: limited physiological reserves, co-morbidities, medications
- Obese: intubation , ultrasound, diagnostic peritoneal lavage & CT scan are difficult. Limited cardiopulmonary reserve.
ILO’s
At the end of this presentation students will be able to describe:
- Incidence of trauma
- Causes & types of trauma
- Timing & mode of death in trauma & its effect on management.
- Pre-hospital care & triage
- Hospital care: Primary survey & initial management
- Secondary survey
- Pathophysiology of common injuries
- Investigations during primary and secondary survey
- A brief outline of management of major injuries.