Pediatrics
Scarlet Fever
Infectious disease caused by group A streptococcus, which is gram-positive cocci, aerobic bacteria. The bacteria infects the throat, produces a toxin → scarlet fever. Most common in children between two and ten years old, it was very serious before, but now easily treatable.
- Streptococcus usually enters the body through the mouth or nose traveling through the respiratory tract.
- It travels through the body and lays between the cells and the skin tissues in most cases.
- Then the bacteria produce a toxin that causes several infections to occur.
- In rare cases, scarlet fever may develop from a streptococcal skin infection like impetigo. In these cases, the person may not get a sore throat.
Transmitting Streptococcus
- Direct contact from person to person: droplets of spray from the infected person or holding hands.
- Indirect contact: touching something that the infected person has touched and used like silverware.
The Incubation Period
It is 1–4 days. Asymptomatic carriage may occur in 15–20% of school-age children.
Symptoms & Signs
- Fever
- Sore throat
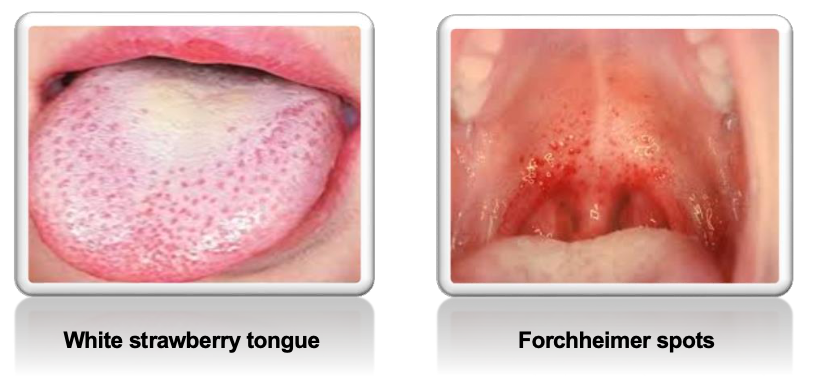
- White strawberry tongue
- Peeling of the skin around the fingertips
- Forchheimer spots: fleeting small, red spots on the soft palate.
Rash: which appears 12 days after the toxin is released into the body and 12-48 hours after the fever.
- The rash starts on the neck and chest and spreads out over the body, fine, tiny, red bumps.
- Blanches upon pressure.
- On the face, often shows as red cheeks with a characteristic pale area around the mouth (circumoral pallor).
- The rash worsens in the skin folds (so-called Pastia’s lines, where the rash runs together in the armpits and groin, can persist after the rash is gone).
- It begins to fade three to four days after onset and desquamation (peeling) begins.


“This phase begins with flakes peeling from the face. Peeling from the palms and around the fingers occurs about a week later.” Peeling also occurs in the axilla, the groin, and the tips of fingers and toes.
- Sandpapery texture: lasts for about a week and then fades slowly - fading may take up to a month.

Diagnosis
- Complete blood count (high WBC with neutrophilia and conserved or increased eosinophils).
- High erythrocyte sedimentation rate and C-reactive protein.
- Elevation of antistreptolysin O titer.
- Throat culture is usually most successful.
- Blood culture is rarely positive.
- The rash is also important in diagnosis – the texture is more important than the look.
Complications
- It is due to the spread of streptococci in blood, and immune-mediated complications due to an aberrant immune response.
- Septic complications—today rare—include: ear and sinus infection, streptococcal pneumonia, empyema thoracis, meningitis, and full-blown sepsis (malignant scarlet fever).
- Immune complications include:
- Acute glomerulonephritis.
- Rheumatic fever.
- Erythema nodosum.
 erythema nodosum
erythema nodosum
Treatment
-
George Fredrick Dick developed the vaccine in 1924 (discontinued due to poor efficacy and the introduction of antibiotics).
-
Penicillin was then developed in the 1940s.
-
A person with scarlet fever should not be infectious after 24 hours on antibiotics.
ENT
Cause:
Endotoxin from type A B-hemolytic streptococcus
Symptoms:
- red pharynx
- strawberry tongue
- perioral skin erythema and desquamation
- Dysphagaia
- Malaise
- sever cervical lymphodenopathy
Diagnosis:
Throat culture
Treatment:
Antibiotics

