Common Adult Injuries Spine

Prof. Mamoun Kremli

Objectives
- Revision of Anatomy
- Principles of spine injury
- Differentiation between:
- Stable & Unstable injuries
- Common injuries of:
- Cervical – Thoracic – Lumbar
- Treatment
Basic Anatomy
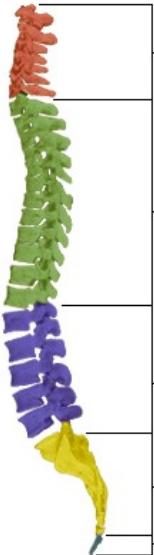
Spinal Column Structure
Cervical Vertebrae
- Number: 7
- Range: C1 - C7
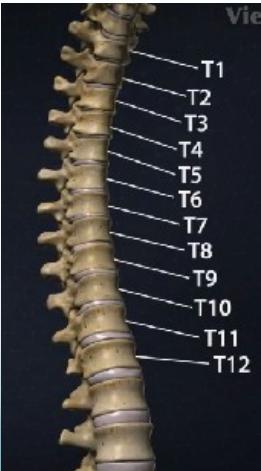
Thoracic Vertebrae
- Number: 12
- Range: T1 - T12
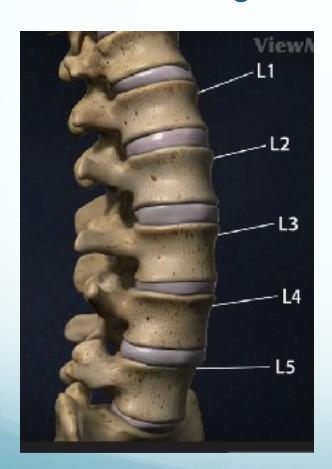
Lumbar Vertebrae
- Number: 5
- Range: L1 - L5
Sacrum
- Number: 5 (fused)
Coccyx
- Number: 4 (fused together)
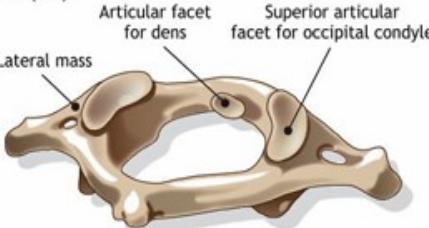
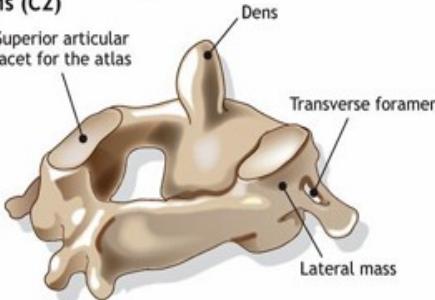
Special Vertebrae
Atlas (C1)
Axis (C2)
Regional Spine Characteristics
Thoracic Spine
- Lower thoracic not protected by ribs / more mobile

Lumbar Spine
- Main weight-bearing – very mobile
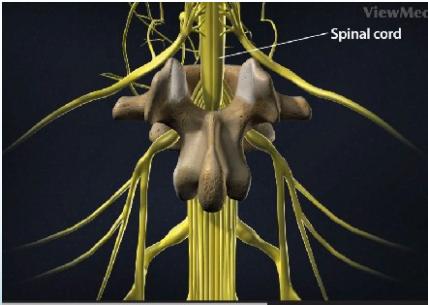
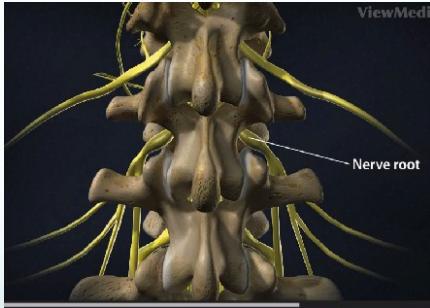
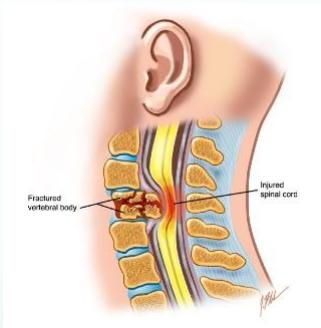
Spinal Cord and Roots
- Spinal cord in spinal canal – spinal roots
Structural Elements
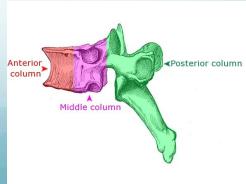
Three-Column Classification System
- Posterior column:
- Pedicles, Facet joints, Posterior bony arch, Interspinous and Supraspinous ligaments
- Middle column:
- Posterior of vertebral body, Posterior part of IV disc, Posterior longitudinal ligament
- Anterior column:
- Anterior of vertebral body, Anterior part of IV disc, Anterior longitudinal ligament

Types of Spine Injuries
Classification Overview
- Double threat:
- Damage to vertebral column & to neural tissue
- Stable: (90%)
- Less risk of displacement
- Little risk of neural elements damaged If it initially undamaged
- Unstable: (10%)
- Unstable if:
- Fracture of middle column + one more column
- Risk of displacement / further damage to neural tissue
Mechanism of Injury
Direct Injuries
- Penetrating injuries: firearms & knives
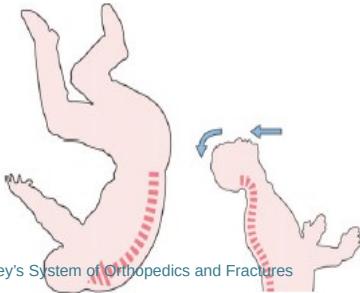
Indirect Injuries (more common)
- Traction: avulsion fractures
- Falls & violent free movements
- Axial/lateral Compression
- Flexion/Extension
- Rotation
- Shear
Suspicion of Spinal Injury
High-Risk Scenarios
- Head injury
- Loss of consciousness
- Severe facial injuries
- Blunt injury above clavicle
- Pain/stiffness in neck/back
- Fall from height
- Crushing accident
- High-speed deceleration
- Neurological symptoms in limbs
- Rib fractures or seat belt bruising
- Severe abdominal/pelvic and injuries

Cervical Spine Region

Thoracolumbar Spine Region
Principles of Management
Key Principles
- Diagnosis and management go hand in hand
- Follow ATLS protocol: ABC
- Inappropriate movement & examination worsen the injury
- Must immobilize the spine If any suspicion of spinal injury
Examination
Primary Assessment
- Look:
- General, attitude, bruises on head, face, back
- Feel:
- Tenderness, swelling
- Do NOT Move

Apley’s System of Orthop and Fr
Apley’s System of Orthopedics and Fractures
Log-Roll Technique
- Protect spine
- Log-roll patient to see back

Apley’s System of Orthop and Fr


Apley’s System of Orthopedics and Fractures
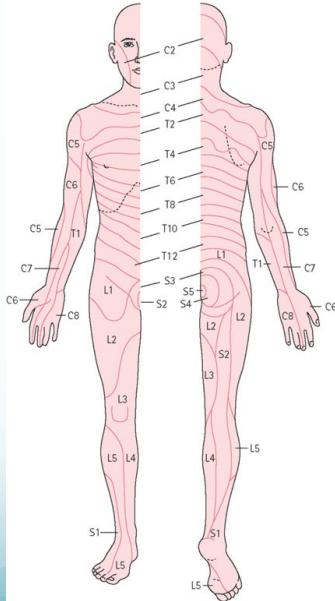
Neurological Examination
Comprehensive Assessment
- Full neurological examination is a must
- Dermatomes
- Myotomes
- Reflexes
- To be repeated over days
Imaging
Standard Views
- C-Spine:
- AP – Lateral – Open-mouth
- T and L-Spine:
- AP – Lateral
- Plain X-rays alone insufficient to show the true picture
Advanced Imaging
- CT for difficult areas (upper/lower C, upper T)
- Shows structural damage of vertebrae and vertebral fragments into the canal
- MRI the best to show:
- IV disc, Ligamentum flavum, Neural structures
Important Limitation
- Plain X-rays alone may be insufficient to show the true picture
X-rays for C-Spine Injuries
AP View
- Intact lateral outline
- Spinous processes & Trachea in the middle
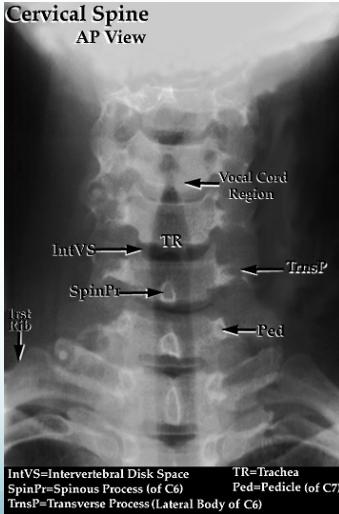
Key Anatomical Landmarks:
- IntVS = Intervertebral Disk Space
- SpinPr = Spinous Process (of C6)
- TrnsP = Transverse Process (Lateral Body of C6)
- TR = Trachea
- Ped = Pedicle (of C7)
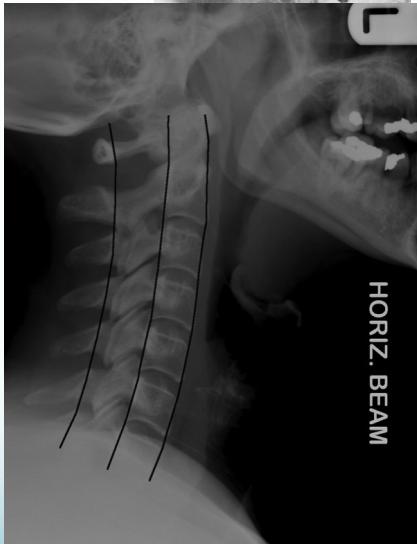
Lateral View
- All C- vertebrae & upper T1
- Prevertebral soft tissue width
- Four parallel curves
- Front of vertebral bodies
- Back of vertebral bodies
- Posterior borders of lateral masses
- Bases of spinous processes
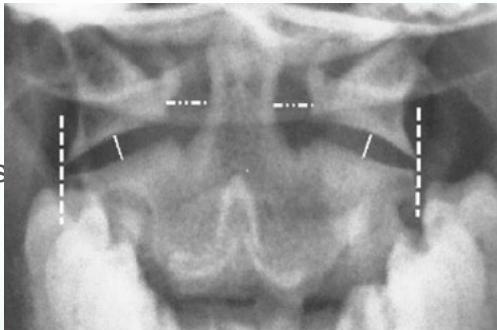
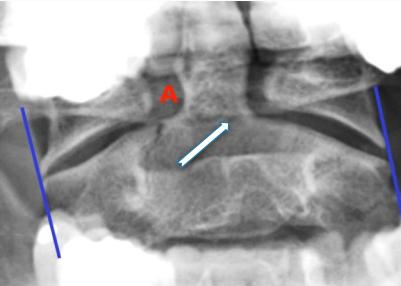
Open-Mouth View
- For C1 and C2
- Odontoid fractures
- Lateral mass fractures
- Look for:
- Symmetry
- Continuity of bone
Treatment
Treatment Factors
- Stable / Unstable
- With / without neurological injury
Objectives of Treatment
- Preserve neurological function
- Relieve reversible neural compression
- Restore alignment of spine
- Stabilize the spine
- Rehabilitate the patient
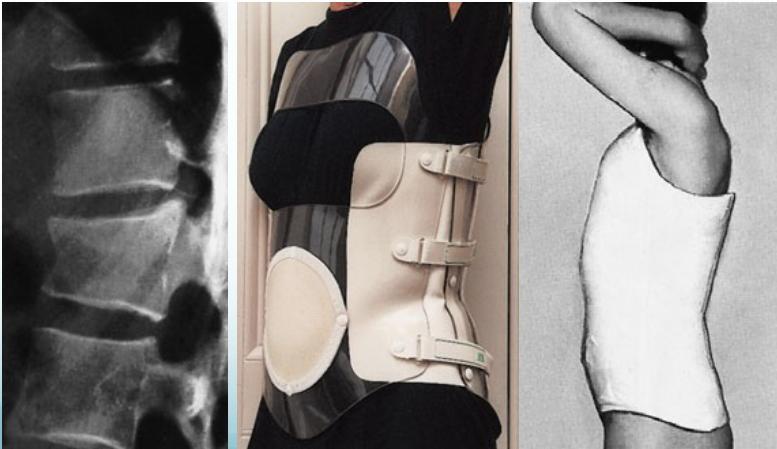
Stable Without Neurological Injury
- Conservative (support by orthotics, rest)




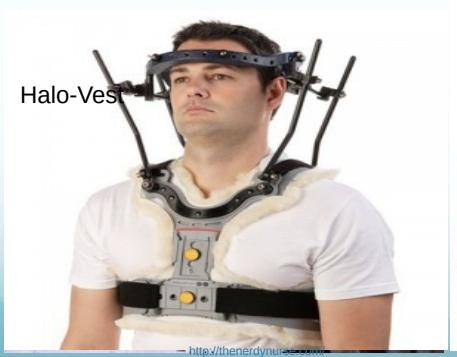
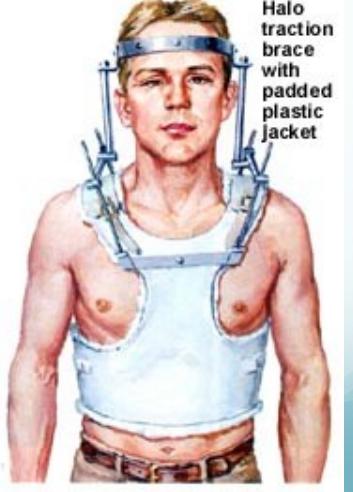
Unstable With/without Neurological Injury
- Secure stabilization:
- Skin / Skeletal Traction
- Surgery +/- Decompression
Comprehensive Treatment Approach
- Unstable With/without Neurological Injury:
- Secure stabilization:
- Skin / Skeletal Traction
- Surgery +/- Decompression
- Secure stabilization:

Specific Fractures
Fractures of C2 (Hangman’s Fracture)
- Hyperextension/distraction injury
- In MVA when forehead strikes dashboard
- Unstable
- May cause death (why?)

discontinuity of the central axial spinal pillar

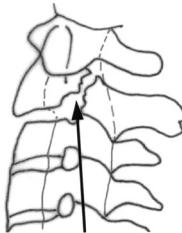
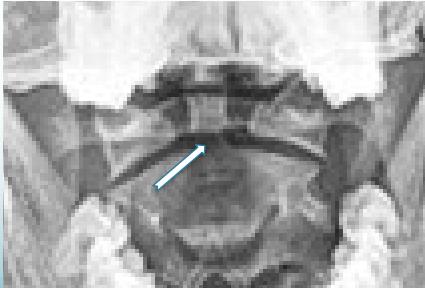
Fractures of C2-Odontoid
- Identified easily by:
- Open mouth view
- CT scan
www./ortho-teaching.feinberg.northwestern.edu/
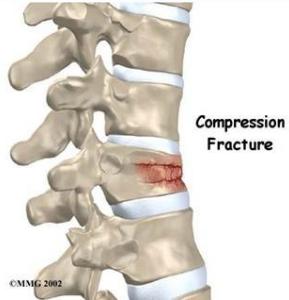
Cervical Wedge-Compression Fracture
- Pure flexion injury
- Mid- & lower cervical
- Stable if only anterior column affected

Cervical Burst Fracture
- Axial compression
- Diving
- Unstable
- Neurological injury


http://www.learningradiology.com/
Fracture-Dislocation
- Flexion-Rotation
- Articular facets ride forwards over facets below
- Usually with fracture of articular mass
- Unilateral facet: stable
- Displacement < 25% of vertebral body width
- Bilateral facet: Unstable
- Displacement > 25% of vertebral body width

Sprained Neck (Whiplash Injury)
- Soft tissue sprain only - stable
- RTA: Rear-end collision:
- Body thrown forwards, neck jerked backwards
- Pain/stiffness over 48 hours
- Treatment:
- Pain relief
- C-Collar
- Physiotherapy

Thoracic Spine Injuries
Wedge Compression
- Common in osteoporotic spine
- Mild trauma to old lady
- Usually stable
- Causes ↑kyphosis
Severe Injuries in Young
- More in T11, T12 (not protected)
- May cause neurological injury
Upper T-Spine
- Lateral not clear
- Need CT

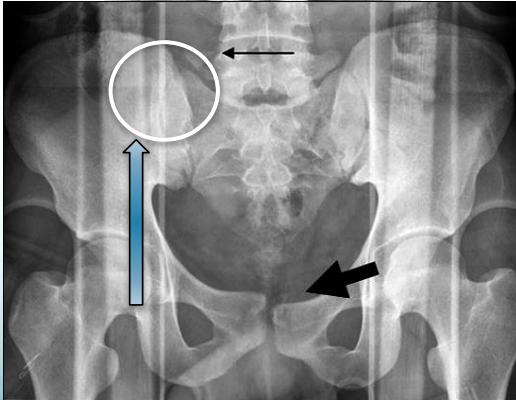
Transverse Processes Fracture
- Avulsion fracture of Transverse Processes
- Isolated, stable
- Supportive treatment
- Fracture of L5 transverse process (Red flag)
- Might indicate a shear injury of pelvis

Lumbar Spine Injuries
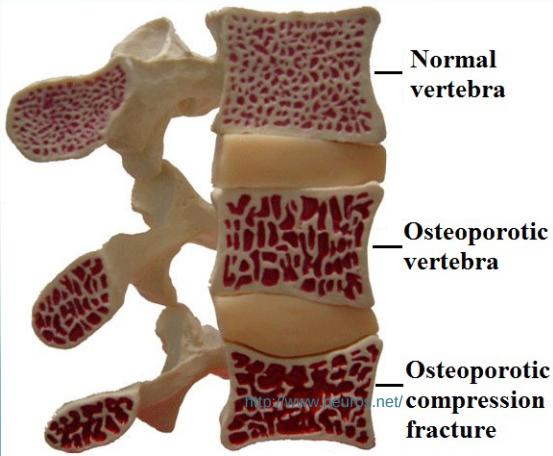
Wedge Compression L-Spine
The Commonest Vertebral Injury
- Minor trauma in osteoporotic people
Normal vertebra
Osteoporotic vertebra
Osteoporotic compression fracture

Stable Compression (posterior elements intact)
- Anterior vertebral body height reduced by < 50%
Unstable Compression (posterior elements injured)
- Anterior vertebral body height reduced by > 50%

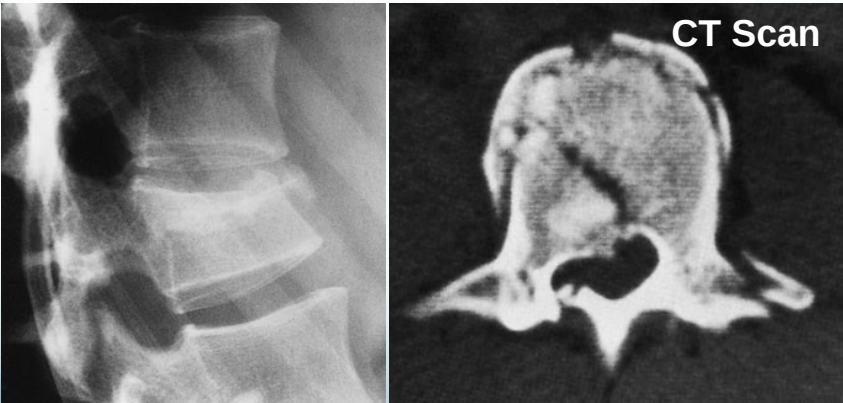
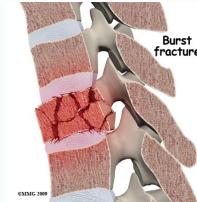
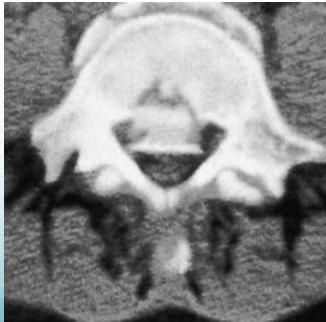
Burst Injury L-Spine
- Axial compression: shattered vertebral body
- Posterior fragments into spinal canal
- Usually unstable
- CT required

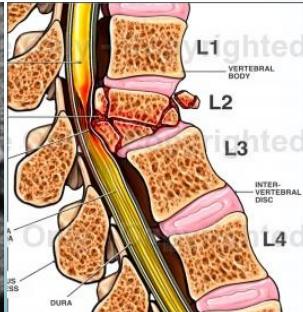
Burst Injury Classification
Is this a compression or a burst fracture?
- A burst fracture
- Why?
- Posterior displacement

Neurological Injuries
C4 Injury
- Quadriplegia/Tetraplegia
- Results in complete paralysis below the neck
7 Cervical Vertebrae
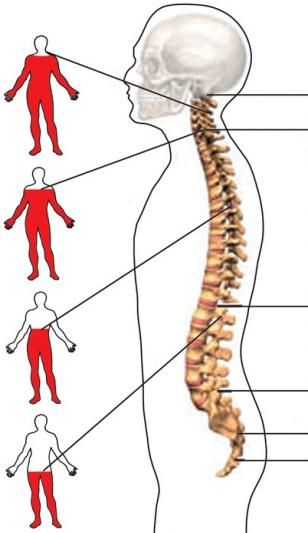
C6 Injury
- Results in partial paralysis of hands and arms as well as lower body
12 Thoracic Vertebrae
T6 Injury
- Paraplegia, results in paralysis below the chest
L1 Injury
- Paraplegia, results in paralysis below the waist
5 Lumbar Vertebrae
5 Sacral Vertebrae
4 Coccyx (fused together)
Summary
- Vertebral injuries are common
- Stable VS. Unstable
- Which column(s) are injured
- Forces:
- Axial compression, flexion, shear, combinations
- Imaging:
- X-rays: AP, Lateral, Special views
- Always assess neurological status