It is due to obstruction of gallbladder from an impacted stones in the neck of gallbladder or cystic duct resulting in a chemical inflammatory reactions that may superimposed by bacterial infection (mainly E. Coli, Klebsiela aerogenoses), usually it start as biliary colic. The thickened gallbladder wall becomes intensely inflamed, edematous and occasionally gangrenous. The fundus of distended, inflamed gallbladder may perforate, giving rise to localized abscess formation and occasionally to biliary peritonitis.
Symptoms:
Sever persistent abdominal pain, mainly in the right upper quadrant radiating to the right subscapular region, associated with tachycardia, pyrexia, nausea, and vomiting. The pain in acute cholecystitis is usually constant and continue for 24 hours or more differentiating this from biliary colic where the pain is short-lasting.
Signs:
Abdominal tenderness and rigidity may be generalized but are most marked over the gallbladder. Boas,s sign (hyperesthesia over the region around the tip of the right scapula) and Murphy’s sign (a catching of the breath at the height of inspiration while the gallbladder area is palpated) are usually present. A right hypochondrial mass may be felt. This is due to omentum ‘wrapped’ around the inflamed gallbladder. The development of a tender mass, associated with rigors and marked pyrexia, signal empyema formation. The gallbladder may become gangrenous and perforate, giving rise to biliary peritonitis. Jaundice can develop during the attack. Usually due to associated stone in the common bile duct but gallbladder may be compressed by enlarged gallbladder or due to severe edema in porta hepatis.
Differential diagnosis
- Perforated peptic ulcer
- High retrocaecal appendicitis
- Acute pancreatitis
- Myocardial infarction
- Basal pneumonia
Investigations
Blood tests: will show high white blood count (leukocytosis ++ FEVER), sometime high liver function test due to the edema in the porta haptis compressing the extra-hepatic biliary tract.
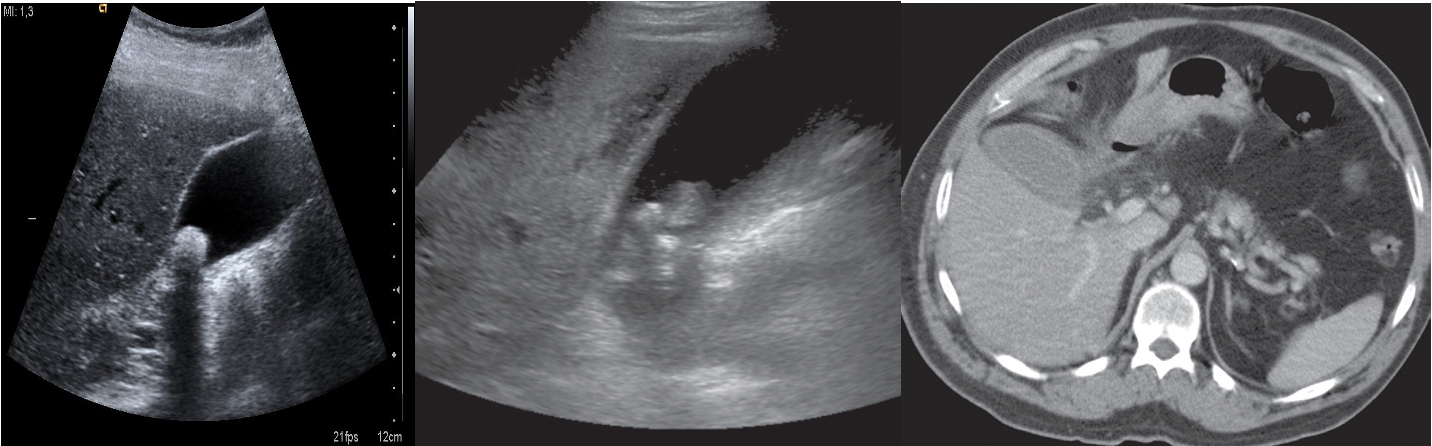
Imaging: Ultrasound abdomen will show distended gallbladder with thick wall, peri-cholecystic fluids and positive ultrasound prop Murphy’s sign.
Treatment
- Admission to the hospital
- Nothing given by mouth
- Intravenous fluids infusion
- Intravenous antibiotics
- Analgesia
- Surgery: Cholecystectomy if the patient presented within 3 days from the onset of the symptoms, otherwise should be managed conservatively and interval cholecystectomy after 2 – 3 months