Prevalence:
More common in females over 40 years old.
Symptoms:
- Progressive dysphagia, first to solids then to fluids.
- Hoarseness of voice and stridor due to invasion of larynx or recurrent laryngeal nerve.
- Neck mass due to nodal metastasis.
- Referred pain.
- Loss of weight.
Signs
- Moure’s Sign: Absence of laryngeal click.
- Cervical Lymph Node: Usually enlarged, unilateral, hard, fixed to deep structures.
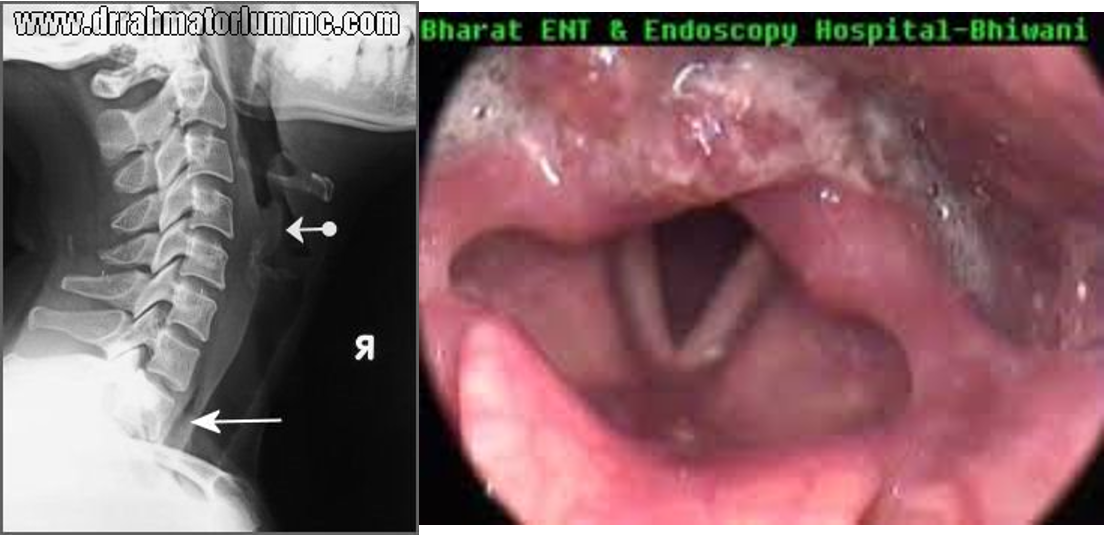
- Indirect Laryngoscopy: Tumor seen behind the arytenoids covered with froth. May affect vocal cord mobility.
Investigations
- Lateral X-ray: Shows widening of the tracheo-vertebral space.
- Barium Swallow: Shows filling defect or obstruction.
- CT and MRI: Show extension, invasion, and LN involvement.
- Biopsy: By hypopharyngoscopy.
- Metastatic Workup: Plain X-ray chest, CT brain, and abdominal ultrasound.
Treatment
-
Surgical: Layngo-pharyngectomy and block dissection. Phx. is reconstructed by Myocutaneous flap,Colon or Jujenuminterposition or Stomach pull up.
-
Irradiation