Hypernatremic Dehydration
- Na level is more than 145 meq/L
Presentation
-
May be nonspecific: irritable, lethargic, with doughy skin and a high-pitched cry, eventually having seizures
-
CNS signs are first to develop due to intracellular dehydration of neurons
Replacement
-
Done slowly over 48 hours with the aim of a fall in serum Na of less than 0.5 mmol/L/hr.
-
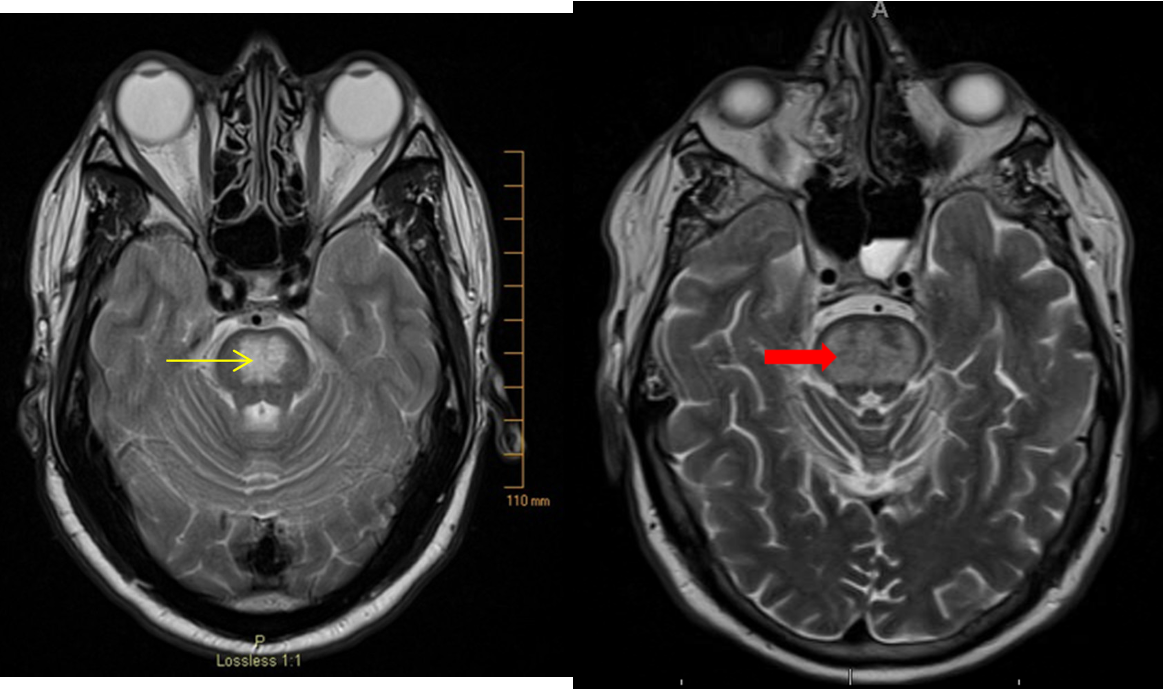
Goal is to avoid a rapid drop of the serum Na+, which is a risk factor for central pontine demyelination and manifests as seizures Z.
Causes
Water and Sodium Loss
- Gastroenteritis
- Burns
- DM
Water Deficit
- DI
- Phototherapy
- Inadequate intake (failed breastfeeding)
Excessive Sodium Intake
- Inappropriately prepared infant formula
- Salt poisoning
- Hypertonic IV
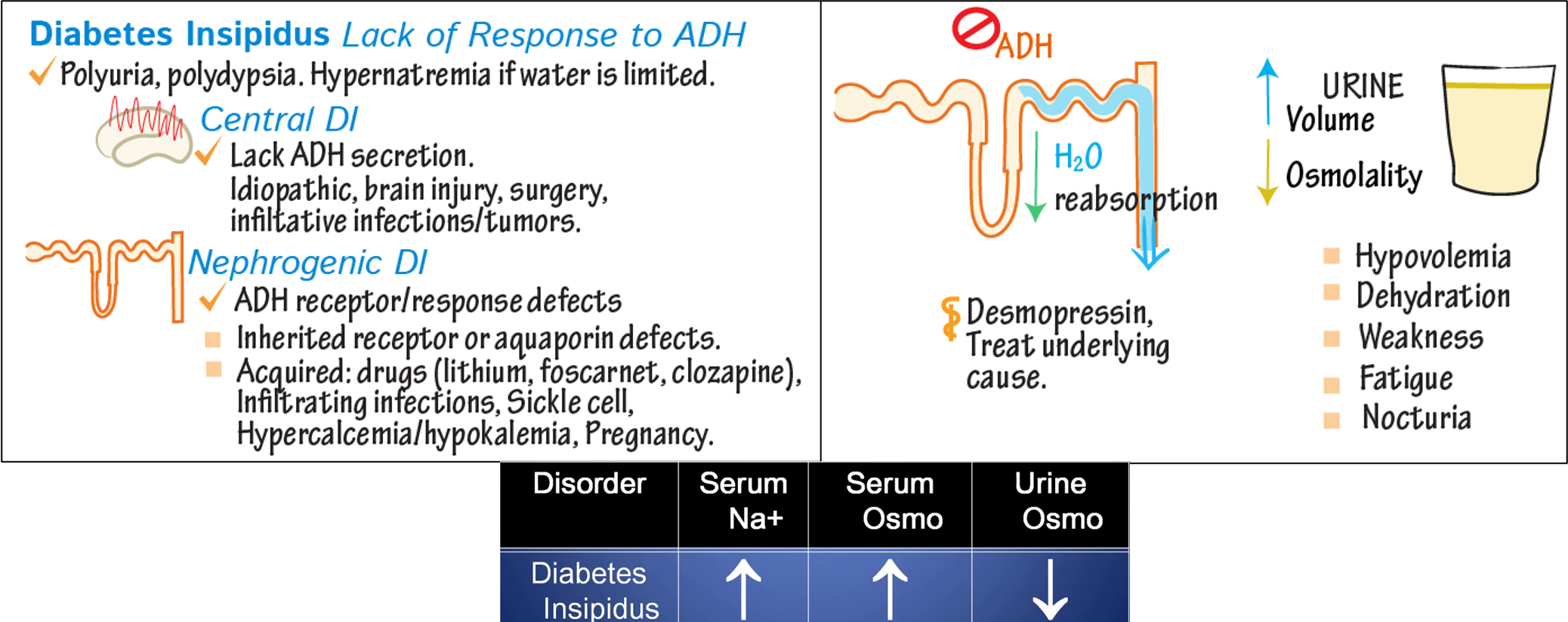
Lack of Response to ADH
- Polyuria, polydipsia: Hypernatremia if water is limited.
Central DI
-
Lack of ADH secretion.
-
Causes: Idiopathic, brain injury, surgery, infiltrative infections/tumors.
Nephrogenic DI
-
ADH receptor/response defects
-
Causes: Inherited receptor or aquaporin defects, acquired (drugs like lithium, foscarnet, clozapine), infiltrating infections, sickle cell, hypercalcemia/hypokalemia, pregnancy.