Primary
- increased secretion aldosterone due to functional tumor
- independent of physiological stimulus
- more often in female
- associated with pheochromocytoma, primary hyperparathyroidism or acromegaly
Secondary
- increased plasma levels of renin
- associated with reno-vascular HTN
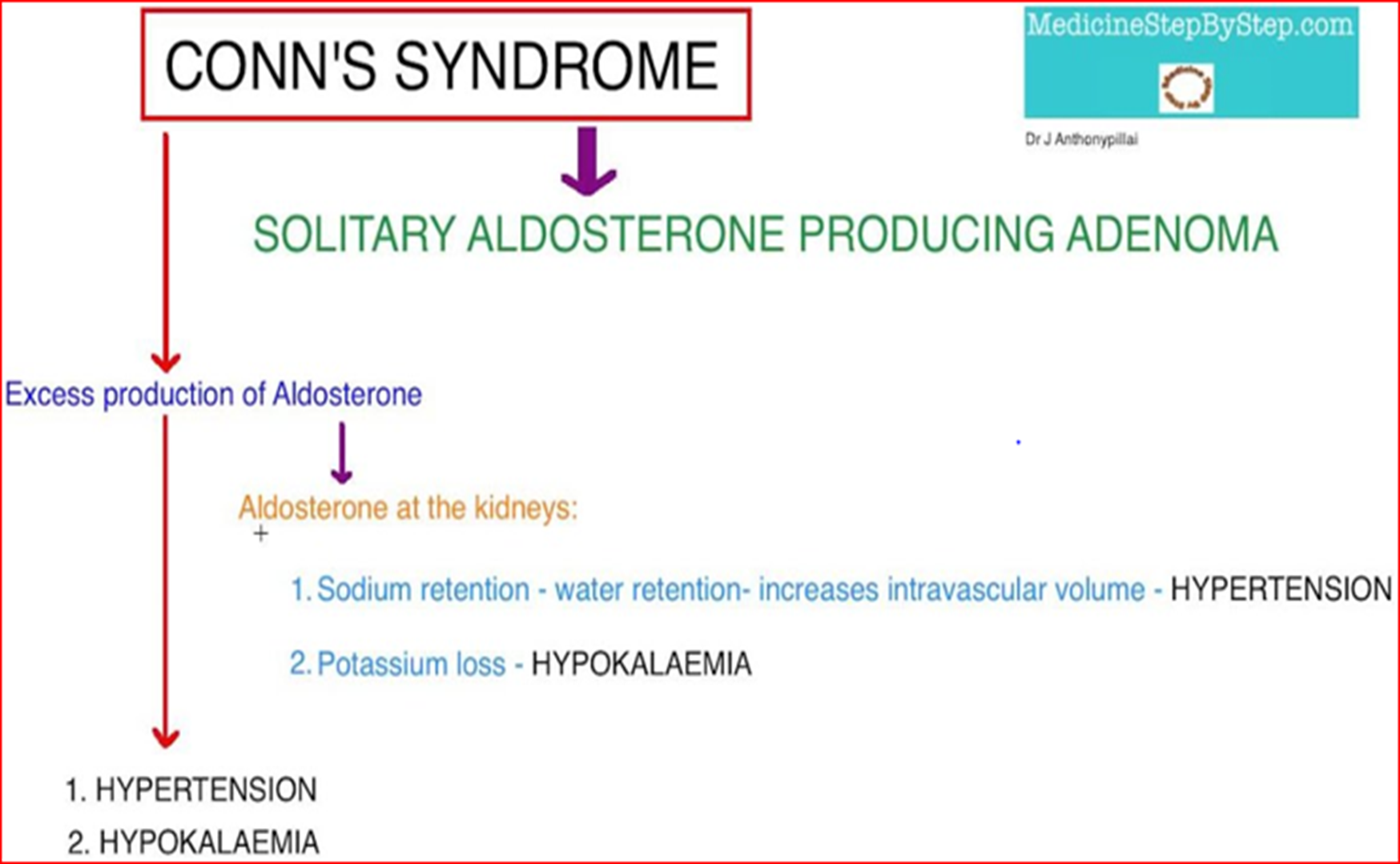
“Conn’s Syndrome”
Too much aldosterone secretion Usually caused by an adrenal tumor
SYMPTOMS & SIGNS:
- High Na and water retention
- HTN
- Low K+
- Usually no edema
Diagnosis:
- High urinary K+
- High plasma aldosterone level with low plasma renin
- EKG changes
- CT scan
Treatment:
- Control BP
- Using Aldactone which is an aldosterone antagonist.
- Correct hypokalemia/hypernatremia
- K+ supplements+ low Na diet
- Partial or total adrenalectomy
The lack of LL edema in Conn’s Syndrome results from spontaneous natriuresis and diuresis (called the “aldosterone escape”) that occurs in patients with primary aldosteronism and that appears to be mediated by atrial natriuretic peptide (ANP)
Nephrogenic diabetes insipidus, caused by reversible hypokalemic tubular damage and renal tubule antidiuretic hormone resistance due to the hypokalemia, can cause nocturia, polyuria, and polydipsia in Conn’s Syndrome
Which hormone is primarily responsible for regulating blood pressure and electrolyte balance?
- Cortisol
- Aldosterone
- Epinephrine
- Insulin
Aldosterone. It helps regulate sodium and potassium levels in the blood, which in turn affects blood volume and pressure.