Bacterial food-borne infections
- Enterica
- Food poisoning
- Cholera
- Brucellosis
- Diarrheal diseases
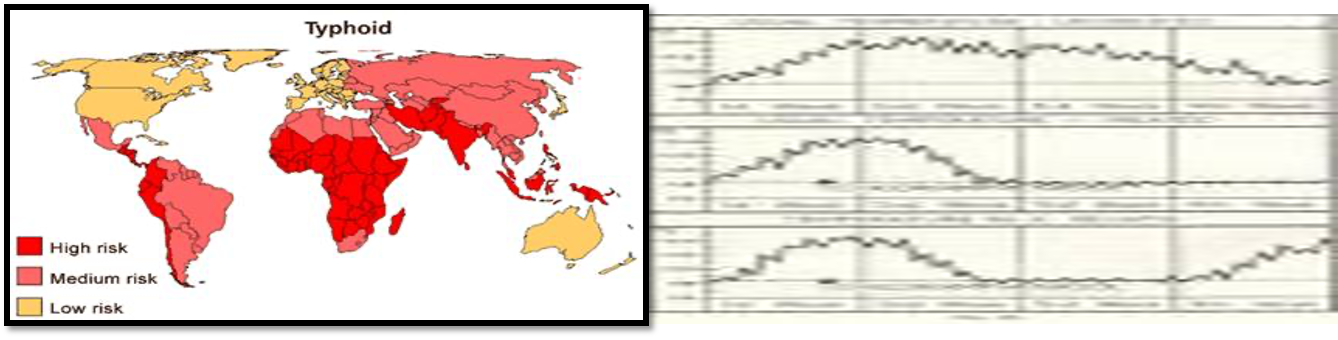
Enteric Fevers (Enterica) Typhoid and Paratyphoid
Causative agent:
Salmonella Typhi Gram-negative facultative anaerobe Bacilli
Modes of transmission:
-
Ingestion of food (vegetables , fish & shellfish)or water contaminated by a. Handling : feces or urine of cases and carriers (Food Handlers). b. Vector: flies-cockraoches c. Dust: food exposed to contaminated dust
-
Direct hand to mouth infection.
Pathogenesis of typhoid
-
The bacteria enter human digestive tract, penetrate intestinal mucosa and multiply in mesenteric lymph nodes, passes into blood ⇒ Bacteriaemia usually within the first week.
-
The Bacteriaemia is temporary and the organism finally lodging in gall bladder.
-
Organisms are shed into the intestine for some weeks.
Virulence factors
- Release of endotoxin and exotoxins.
- Salmonella strains may produce a thermolabile enterotoxin.
Clinical Picture
Classic untreated cases
(1) Prodromal (invasion) stage: (1 week).
- Fever (stepladder rise) &gradual onset sustained fever is usually higher in the evening.
- Pulse: bradycardia (slow relative to fever).
- Constitutional manifestation: malaise, headache, body aches, anorexia , sore throat and cough.
- Rash appears on 6th day.
(2) Advance stage: (2 weeks).
- Continued high fever.
- Worse physical and mental condition.
- Abdominal distension with diarrhea or constipation
Complications (advance stage):
- Ulceration of payers’ patches
- Intestinal hemorrhage: 2nd or 3rd week.
- Intestinal perforation: 3rd week.
- Cholecystitis,meningitis osteomyelitis thrombophlebitis
- Bronchitis and pneumonia.
- Thrombophelibitis (femoral vein).
- Myocarditis.
- Osteomyelitis, bone abscess, spondylitis and non-suppurative arthritis.
- Others: nephritis, meningitis, mental dullness, slight deafness and parotitis.
(3) Decline stage or convalescence: (4th week)
Uncomplicated cases gradually improves
- Temperature decreases .
- Abdominal manifestations disappear with satisfactory general condition.
(4) Relapse: in 10% of untreated cases
It occurs 1-2 weeks after return of temperature to normal.
Management of chronic carriers: Z
Ampicillin 1 gm every 6 hours for 1-3 months or quinolone is found to be effective.
If failed: surgical treatment of the pathological lesion (UB lesions in shistosomiasis, cholecystectomy).
-Should not be released from supervision and restriction until 3 consecutive –ve cultures 1month apart &at least 48 hrs after antimicrobial therapy has stopped
- Patients are probably cured if relapse does not occur within 2 years.
Laboratory diagnosis:
1st week: blood cultures.
- Positive blood culture is conclusive
- (ve+ 75%)but not exclusive
2nd & 3rd week:
- Widal test, stool & urine cultures.
- Bone marrow culture: the best bacteriologic confirmation (90-95%) even in patients received antibiotics.
Differential diagnosis:
- Brucellosis.
- T.B.
- Malaria.