IM
Diabetic Nephropathy
Types:
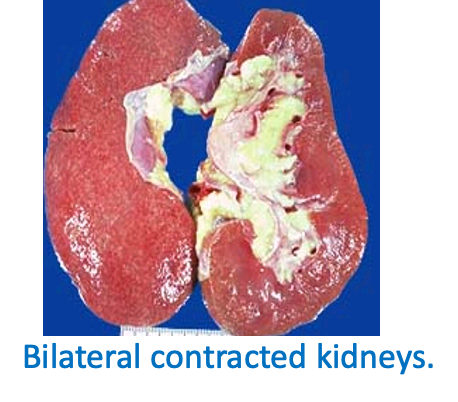
- Most common cause of ESRD (end-stage renal disease)
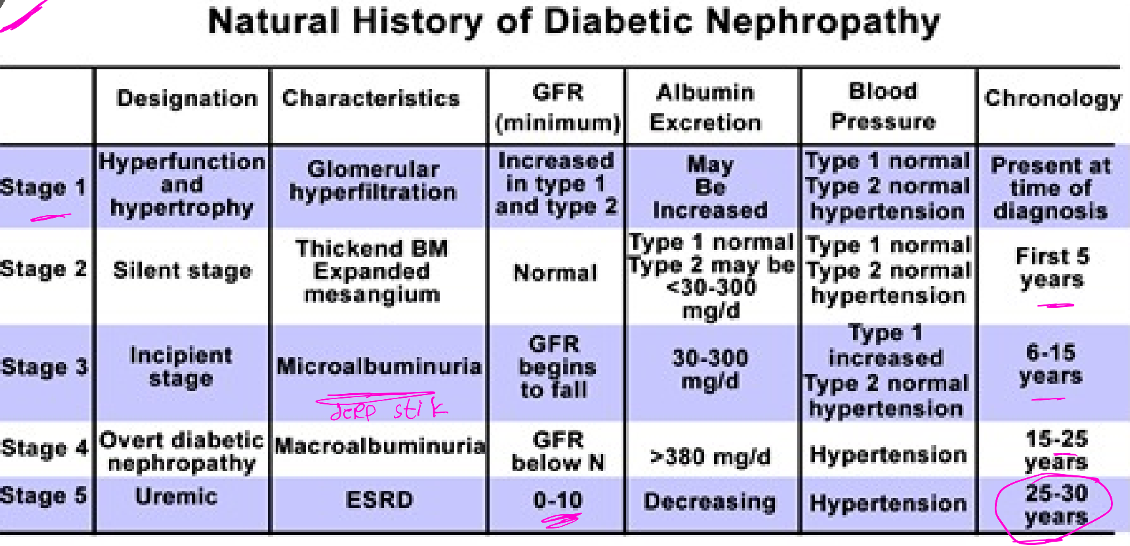
- Starts with microalbuminuria (30-300mg of albumin lost in 24 hrs. urine)
- Progresses to macroalbuminuria (more albumin lost in the urine) finally, causes nephrotic syndrome
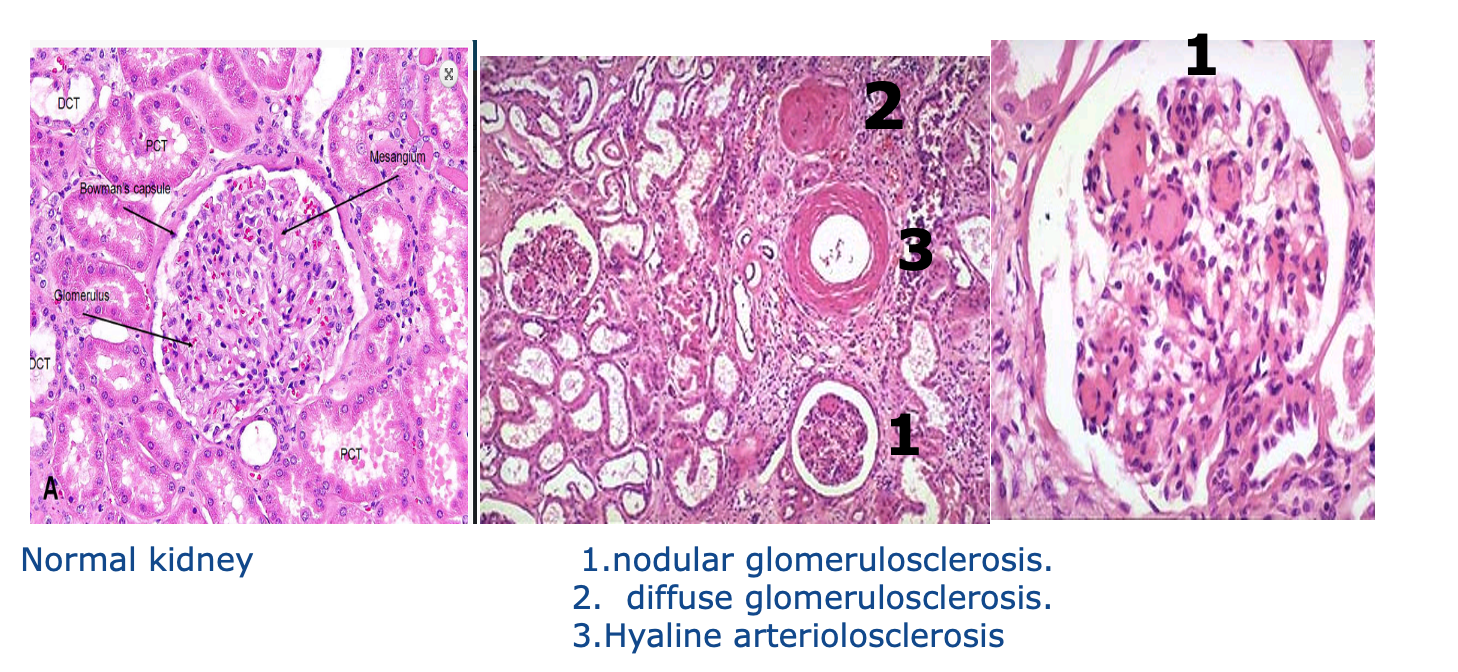
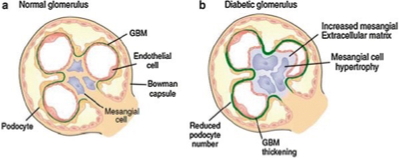
Pathology (biopsy):
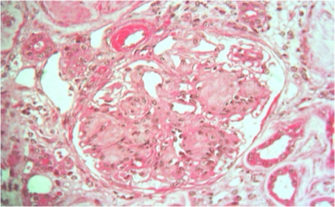
- LM: Sclerosis in the glomerulus & mesangium (Kimmelstein-Wilson nodules). Eosinophilic nodular glomerulosclerosis
- Thick GBM
- No immune deposits
Treatment:
- Strict DM control
- ACE inhibitors (first choice) or ARBs
- Pentoxyphylline & Atrasentan CC?
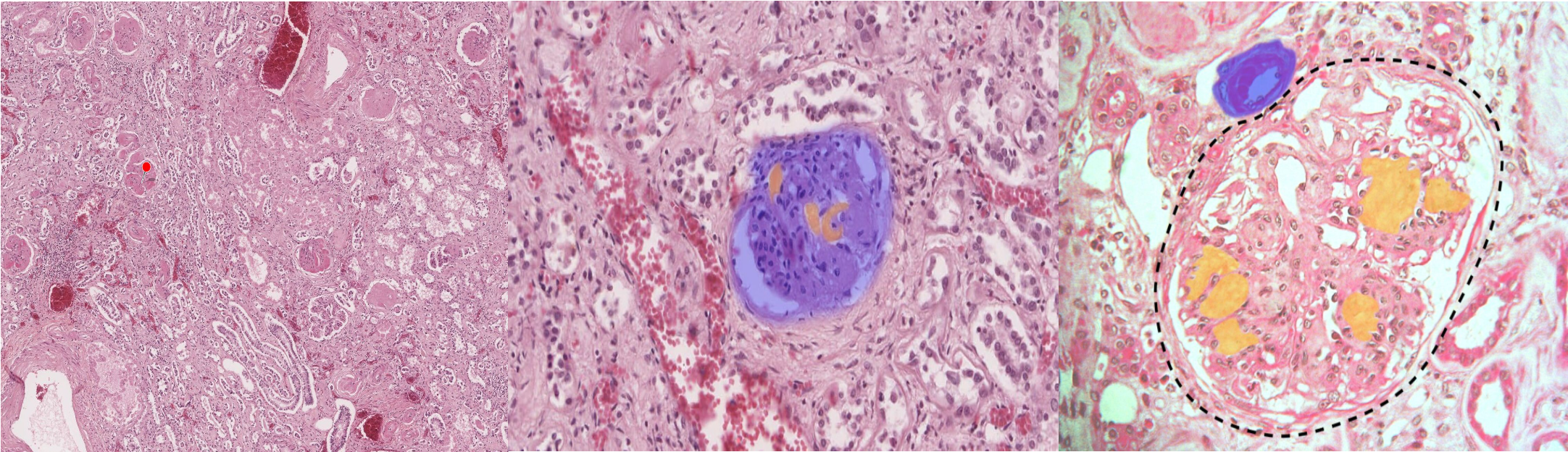 Glomerulus (dashed outline) features a thick basement membrane: contains abundant pink, hyaline agglomerations of PAS-positive material known as Kimmelstiel-Wilson nodules (green overlay). These findings indicate nodular glomerulosclerosis, which is pathognomonic of diabetic nephropathy.
Glomerulus (dashed outline) features a thick basement membrane: contains abundant pink, hyaline agglomerations of PAS-positive material known as Kimmelstiel-Wilson nodules (green overlay). These findings indicate nodular glomerulosclerosis, which is pathognomonic of diabetic nephropathy.
Therapeutic
- About 20 – 30% of patients with diabetes develop diabetic nephropathy.
Pathophysiology: it is 3 stages
1- Hyperglycemia ⇒ increase GFR ⇒ hypertension. (hypertension is also aggravated by activation of renin angiotensin system which cause efferent arteriole vasoconstriction)
2- excess production of reactive oxygen species ,inflammatory cytokines lead to damage of endothelium and increase permeability (albuminuria >300 mg/day).
3-Nephron ischemia (due to damage of mesangial vasculature & vasoconstriction from renin angiotensin system) ⇒ infarction& fibrosis of nephron ⇒ decrease GFR .
Diabetic Nephropathy managment
- Hyperglycemic control
- Antihypertensive drugs
- in end stage with decrease in GFR :
- Renal dialysis.
- Renal transplant.
Microscopic features of diabetic nephropathy
-
Glomerular lesions
-
Nodular glomerulosclerosis: ‘’Kimmelstiel-Wilson lesion’’- nodules in periphery of glomeruli
-
Diffuse glomerulosclerosis.
-
-
Renal vascular lesions -Hyaline arteriolosclerosis in afferent &efferent arterioles -Atherosclerosis in renal artery
-
Pyelonephritis