Surgery
Cold Abscess
Caseation necrosis of cervical lymph nodes.
Why so called? Has no signs of inflammation.
Due to TB lymphadenitis or TB spine (cold abscess in the posterior triangle of neck). but maybe anywhere
Pathology - Stages:
Tuberculous lymphadenitis has 5 stages. Z Clinical Scenario
-
Stage of lymphadenitis
-
Lymph nodes are enlarged, nontender or slightly tender, commonly upper deep cervical nodes are involved.
-
They are discrete and palpable.
-
Age usually 20 to 30 years, i.e. young adults.
-
-
Stage of Peri- adenitis or Matting:
-
Due to involvement of capsule, the nodes move together, become firm and non tender.
-
Matting is pathognomonic of tuberculosis.
-
Other rare causes of matting are chronic lymphadenitis, anaplastic variety of lymphoma.
-
-
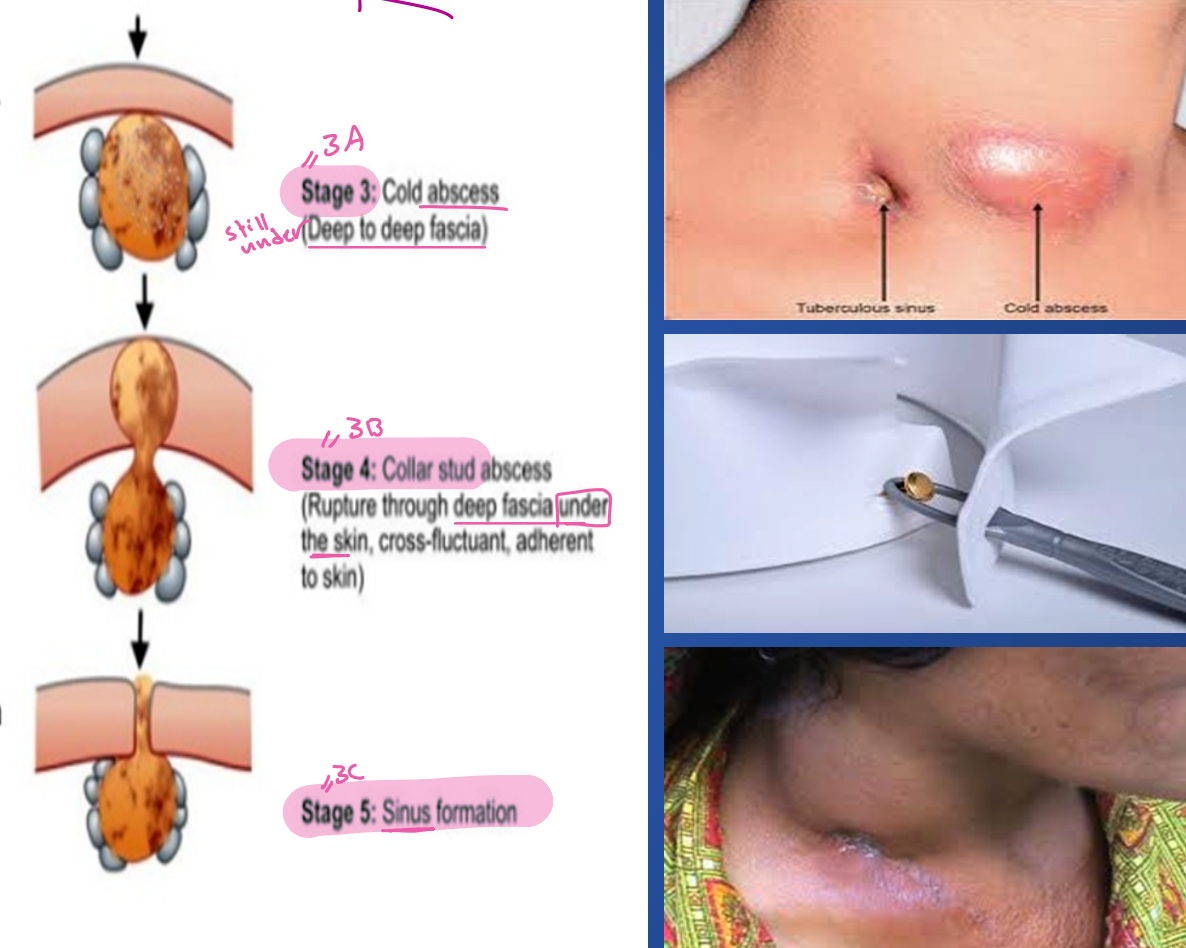
Stage of Cold Abscess (Deep to deep fascia):
-
It occurs due to caseation necrosis of the lymph nodes. The caseating materials liquefies and breaks through the capsules of the lymph nodes to form a ‘cold abscess’.
-
In the beginning, the abscess remains deep to the deep cervical fascia. Ultimately the fascia is eroded at one point and the pus tracks into the superficial space. Now it is called collar stud abscess.
-
The superficial abscess gradually enlarges and becomes obvious on inspection.
-
In untreated cases, the skin at the centre undergoes necrosis and gives rise to the chronic discharging sinus.
-
-
Stage of collar stud abcess (rupture through deep fascia under the skin, cross-flucluantm adherent to skin)
-
Stage of sinus formation
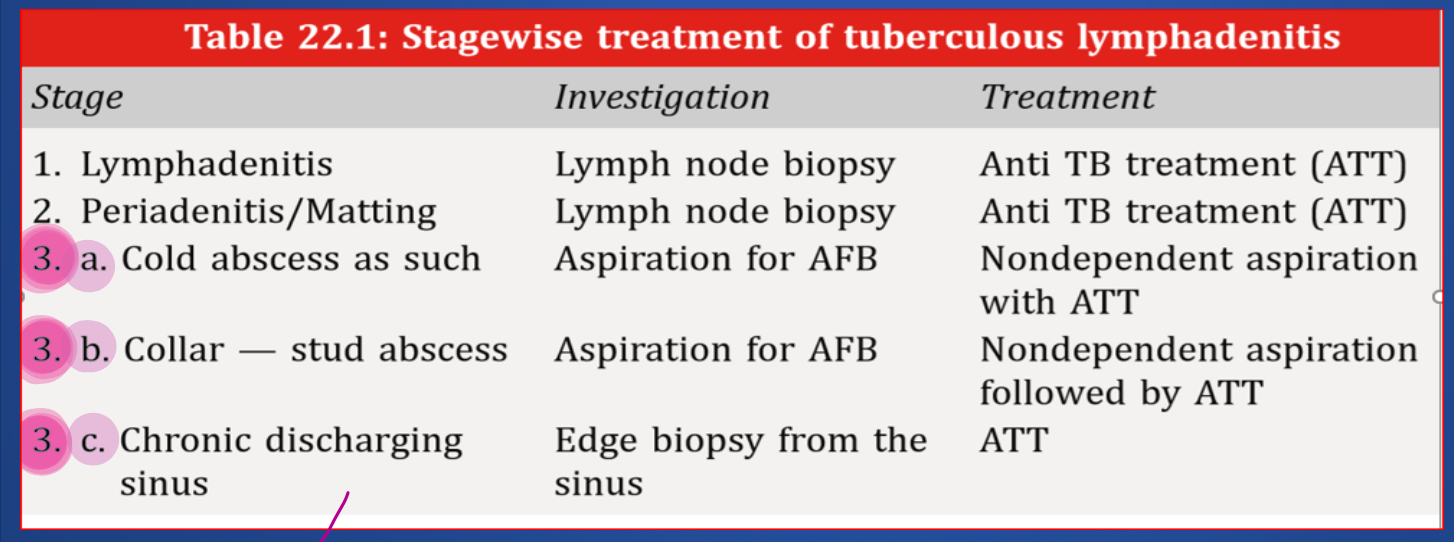
Treatment Plan Based on Stage
initial phases Lymphadenitis & Periadenitis/Matting should be treated with Anti TB medications
When cold abcess or collar stud - Nondependent aspiration with ATT
If chronic discharging sinus ATT
-
Cold abscess is soft, smooth, nontender, fluctuant, without involvement of the skin. It is not warm. This is a clinical manifestation of underlying caseation
-
Left untreated, as a result of increased pressure, cold abscess ruptures out of the deep fascia to form collar stud abscess which is adherent to the overlying skin.
-
Eventually collar stud abscess bursts open, discharging sinus is formed. It can be multiple, wide open mouth, often undermined, nonmobile with bluish color around the edge. It is usually not indurated.
Clinical Features:
Evening rise of temp., Loss of weight, Anorexia, Sweating, Lump in the neck & Tenderness in the cervical spine.
Investigations:
a. CBC (Complete Blood Count) may show low Hb%. ESR is increased in most cases.
b. Chest Xray is usually - ve, sputum is examined for AFB (acid fast bacilli) not nessesory
c. FNAC gives diagnosis in 75 percent cases.
d. Lymph node biopsy reveals central caseation surrounded by epithelioid cells with Langerhan type of giant cells. Z
e. If there is a cold abscess, one can aspirate the content which is cheesy, and may be +ve for AFB.
Differential Diagnosis:
- Branchial cyst-Contains cholesterol.
- Cystic hygroma.
Treatment:
Antitubercular treatment (ATT) for lymphatic TB (Tuberculosis) WHO recommendation for extrapulmonary TB is as follows: The three drug regime INH, Rifampicin, Pyrazinamide (HRZ) for two months followed by INH and Rifampicin for another four months.
Role of Surgery in TB lymphadenitis if there’s bad signs z i. Biopsy-Lymph node biopsy, edge biopsy from the edge of the sinus. ii. Aspiration-Non dependent aspiration of cold abscess. iii. Excision of the lymph nodes, if they persist in spite of ATT. iv. Excision of the sinus along with the tract.

Clinical Medicine
- Caseation necrosis of cervical lymph nodes.
- Why so called ? Has no signs of inflammation.
- Due to TB lymphadenitis or TB spine (cold abscess
- in the posterior triangle of neck).
