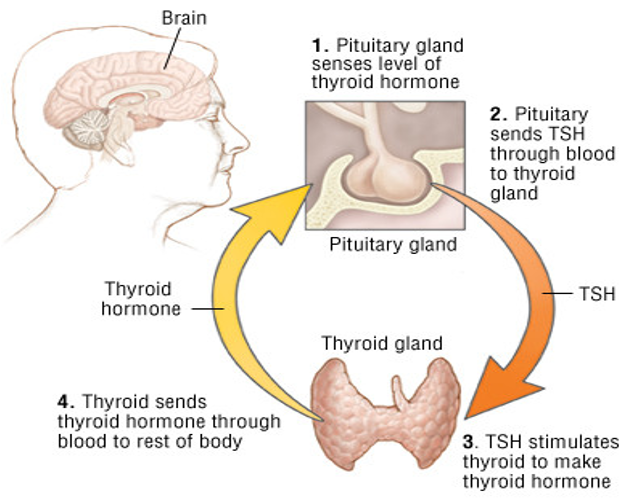
Thyroid Profile:
- TSH (0.4 – 4 mU/L)
- Free T4 (9 – 25 pmol/L) {0.03%}
- Free T3 (3.5 – 7.8 nmol/L) {0.3%}
Free T3 (fT3) is measured, it is less relevant than free T4 (ft4). This is because the thyroid releases T4 and T3 at a ratio of about 20:1 respectively, with T3 (active hormone) mainly being produced by peripheral conversion of T4.
Free T4 (fT4) is roughly 1% of the total T4, with the rest being bound to thyroxine-binding globulin(TBG)
T4 has a half-life of about one week, therefore, to monitor the impact of an intervention (e.g. increasing a patient’s Tab.levothyroxine T4 dose) you need to wait several weeks before repeating TFTs.
Half-life of T3 is only 1-3 days
Hypothyroidism & Hyperthyroidism
Primary hypothyroidism: low T4 and T3 and a raised TSH.
Subclinical hypothyroidism: (caused by autoimmune disease). A normal T4 a raised TSH
Secondary hypothyroidism: Involves a reduction in the hormones that stimulate the thyroid to produce thyroxine. Pathology which affects the pituitary and hypothalamic glands can result in decreased production of TRH and TSH, causing secondary hypothyroidism. The end result is low T4 and T3 and a normal/low TSH.
Primary hyperthyroidism: Excessive production of T3 and T4 by the thyroid gland as a result of pathology within the thyroid gland itself. The end result is a raised T3 and T4 and a low TSH.
Secondary hyperthyroidism: Stimulation of the thyroid gland by excessive thyroid-stimulating hormone (TSH). TSH production is increased by either the pituitary/hypothalamus or another source (known as ectopic production). Raised T3/T4 ; Raised TSH Raised T3/T4: due to excess production that is driven by a raised TSH level. Raised TSH: due to excess production.