Dermatology
Herpes Zoster (Shingles)
4- Herpes zoster
- Herpes zoster is a localized, unilateral eruption
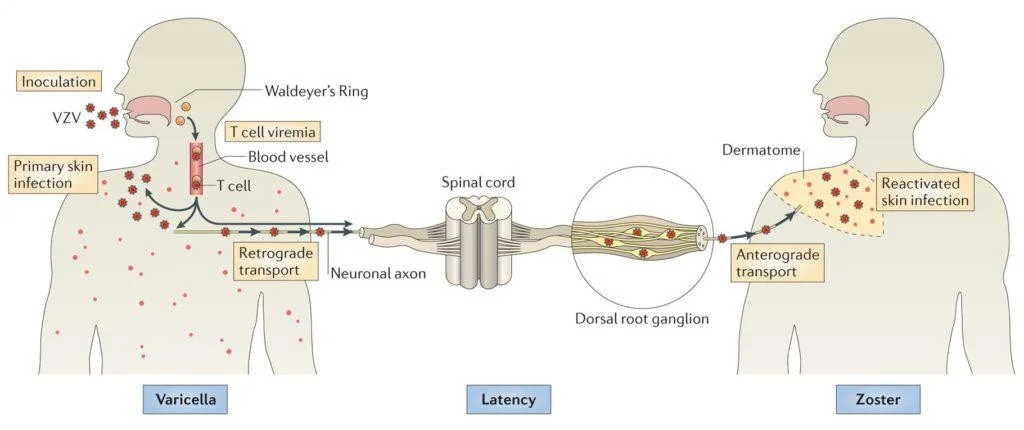
- Varicella-zoster virus is found in the posterior root ganglia of all people who experience a chickenpox infection in the past
- When the immunity of the individual decreases for any reason, the virus reactivated itself.
- HZ is a result of the reactivation of a dormant varicella-zoster virus
- HZ cannot be acquired from another person
Facial, Bilateral presentation of zoster raise red flag to do CBC to exclude malignancies
Clinical features
Prodromal phase
Is dominated by constitutional symptoms:
- Pain, burning, and discomfort in the area of nerve distribution
- Headache, photophobia, fever
Skin lesions
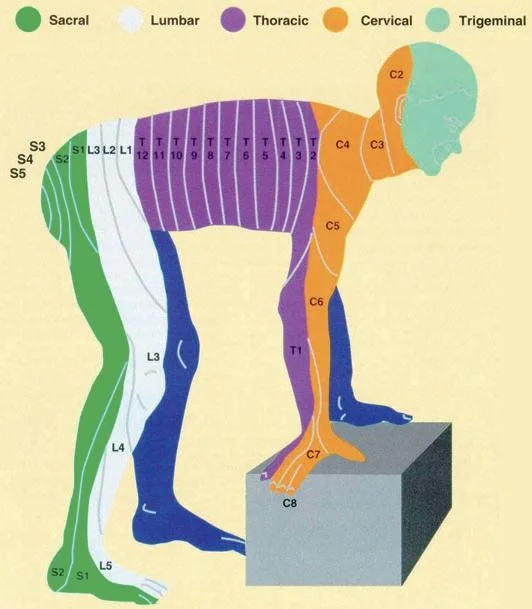
The lesion is usually seen as a band like eruption on one side of the body (dermatomal) mid line cut off.
- Erythema (redness) is first seen in the area followed by papules that rapidly blister






Complication
- Post-herpetic neuralgia is a possible complication
- PHN is a persistent, severe pain after the rash has subsided
- Occurs in 10% to 15% of cases
- Is common in extreme ages especially the elderly.
Treatment
- Topical or systemic antiviral (acyclovir)
- Initiating oral treatment within 72 hours of the onset of HZ can minimize pain and shorten the course of the outbreak.
- Sometimes pain killer medication is prescribed
ENT
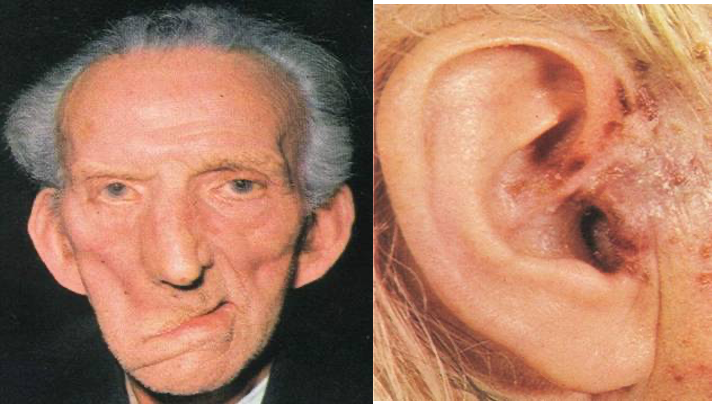
Ramsy hunt syndrome - Herpes zoster otticus
The virus affects the geniculate ganglion of the facial nerve.
C.P. 1- Lower motor neuron facial N. paralysis at level of the geniculate ganglion. 2- Ear pain. 3- Vesicles on the auricle and external auditory meatus. 4- SNHL & Vertigo if 8th nerve is affected.
- Neoplastic: a. Tumors of the middle ear as glomus tumor or carcinoma. b. Acoustic neuroma (neurofibroma of the 8th nerve). c. Neuroma of the facial nerve.
Treatment:
- Acyclovir systemically and locally.
- Analgesic for pain .
- Eye care