(cystadenoma and cystadenocarcinoma.)
-
In some cases it is not possible to say whether the mass is benign or malignant based on the ultrasound, unless there is evidence of local invasion or distant spread.
-
MRI may be used to further characterize indeterminate masses as benign or malignant prior to deciding on patient management.
-
With disseminated malignancy, deposits within the omentum and ascites may be visible , but small omental and peritoneal metastases are frequently difficult to detect.
-
FDG-PET/CT may be used to demonstrate the extent of disseminated disease in order to aid treatment planning.
-
Ultrasound, CT and MRI may show hydronephrosis from ureteric obstruction by the tumour and may also demonstrate -enlarged lymph nodes, liver metastases or pleural effusions.
Morphological features of benign and malignant ovarian masses
| Benign ovarian masses | Malignant ovarian masses |
|---|---|
| Small simple cyst | Large size |
| Thin cyst wall, No solid components | Mixed solid and cystic mass |
| If solid components are seen, then no vascularity is seen on Doppler | Vascularity within solid components on Doppler |
| If septate, then thin and smooth septations | Thickened septations, >3 mm • Bilateral masses • Associated ascites or peritoneal deposits |
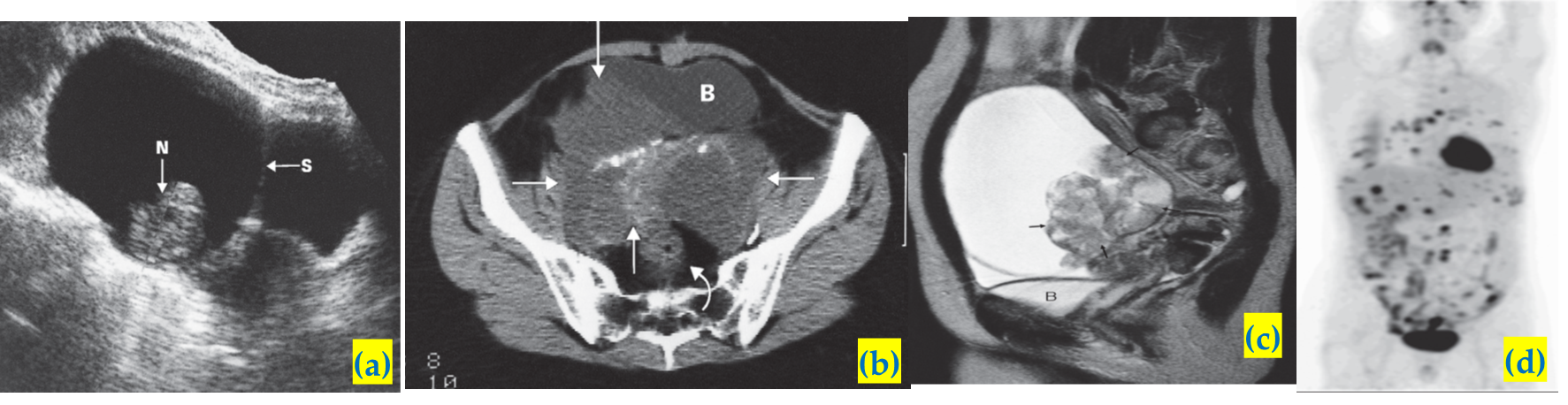
Ovarian carcinoma.
A) Longitudinal ultrasound scan showing a very large multilocular cystic tumour containing septa (S) and solid nodules (N). The lesion was a cystadenocarcinoma..
B) CT scan showing a large partly cystic, partly solid ovarian carcinoma (arrows). The tumour, which contains irregular areas of calcification, has invaded the right side of the bladder (B). The rectum is indicated by a curved arrow.
C) MRI scan showing a partly solid and partly cystic tumour. The cystic component is of high signal intensity on this T2-weighted image.
D) FDG-PET/CT in a patient with disseminated ovarian cancer. Abnormally increased activity is seen in the chest, liver and peritoneum. Normal cardiac and bladder activity is demonstrated