Venous disease
Common presentations:
- Pain in lower limbs
- Prominent veins
- Lower limb swelling
- Skin changes
- Ulcer
- Upper limb pain and swelling
Common venous diseases:
-
* Varicose veins.
-
* Deep venous thrombosis. (DVT)
-
* Superficial thrombophlebitis.
-
* Venous ulcer
-
* Chronic venous insufficiency.
-
* Upper limb pain and swelling.
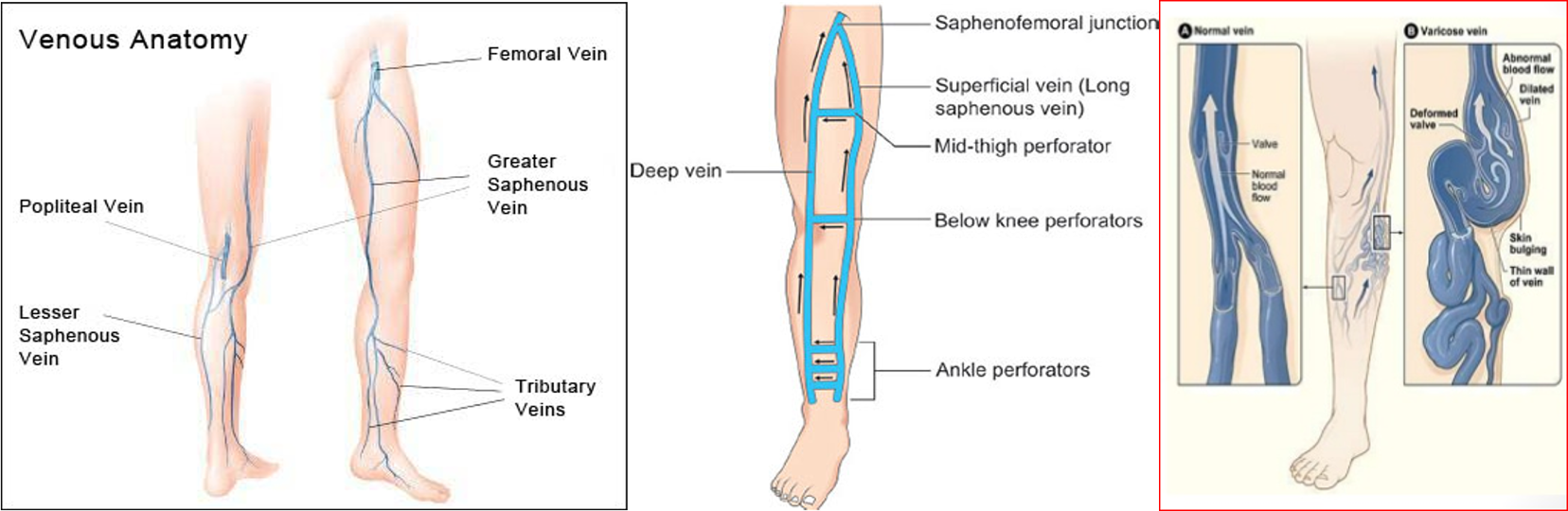
•The GSV- from the dorsal pedal venous arch and courses cephalad and enters the common femoral vein approximately 4 cm inferior and lateral to the pubic tubercle.
•The LSV- originates laterally from the dorsal pedal venous arch and courses cephalad in posterior calf to join the popliteal vein
Multiple perforator veins traverse the deep fascia to connect the superficial and deep venous systems at multiple levels
most common site in ankle
History
Clinical Features:
- Pain (most common),
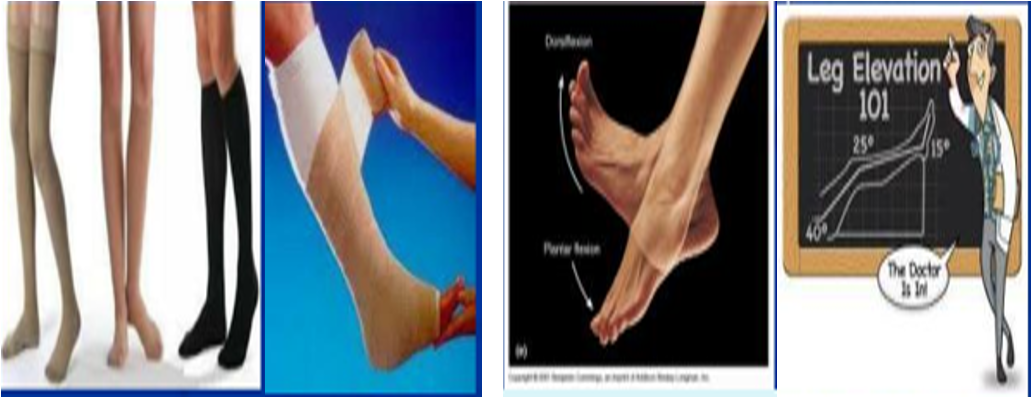
- Ankle and calf oedema – relieved by foot elevation
- Pruritus, brownish hyperpigmentation (hemosiderin deposits)
- Stasis dermatitis, subcutaneous fibrosis if chronic (lipodermatosclerosis) Z
- Ulceration: shallow, above medial malleolus, weeping (wet), painless, irregular outline
- Signs of DVT/varicose veins/thrombophlebitis

History of risk factors
- Female
- Increased age
- Previous thromboembolism
- Malignancy
- Trauma
- Obesity
- Pregnancy
- Post-operative state
- Prolonged recumbency
- Remaining history as any other patient
- Family history of varicose veins
- Use of contraceptive pills
Inspection
-
Both lower limb exposed & compare
-
Supine & standing (for varicose veins)
-
Look for varicose veins ( anterior & posterior)
-
Document the venous system involved
-
Calf or whole limb swelling (duration)
-
Localized swelling and skin changes in superficial thrombophlebitis in the line of superficial vein
-
Features of chronic venous insufficiency (CVI): Oedema, leg induration, pigmentation, eczema, ulceration, skin thickness & redness- lipodermatosclerosis
-
Ulceration: Venous ulcers are located around medial lower 1/3rd of the leg noting size, shape, margin and floor - ankle flare


Palpation
- Temperature: warm (DVT, infection)
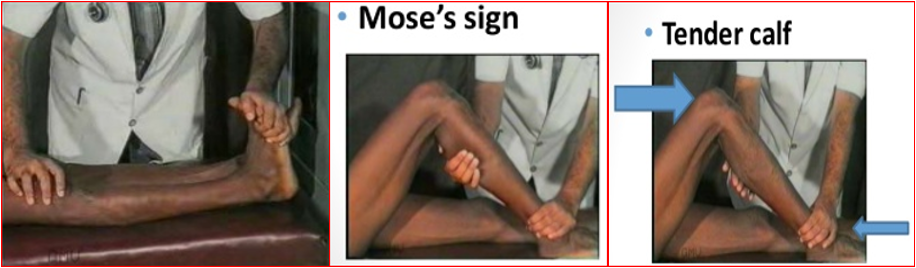
- Tense and tender calf (DVT)
- Cord like structure tender in superficial thrombophlebitis
- Homan’s sign- stretching calf by foot dorsiflexion causes pain
- Fegans’ Method: Defect in deep fascia
- Pitting edema
- Skin thickening, redness
- Groin LNs – cough impulse
- Abdominal masses
Schwartz or Tapping Test
Tapping the venous column demonstrates pressure transmission to incompetent distal veins.
Coughing impulse
at sapheno-femoral junction denotes incompetent valve

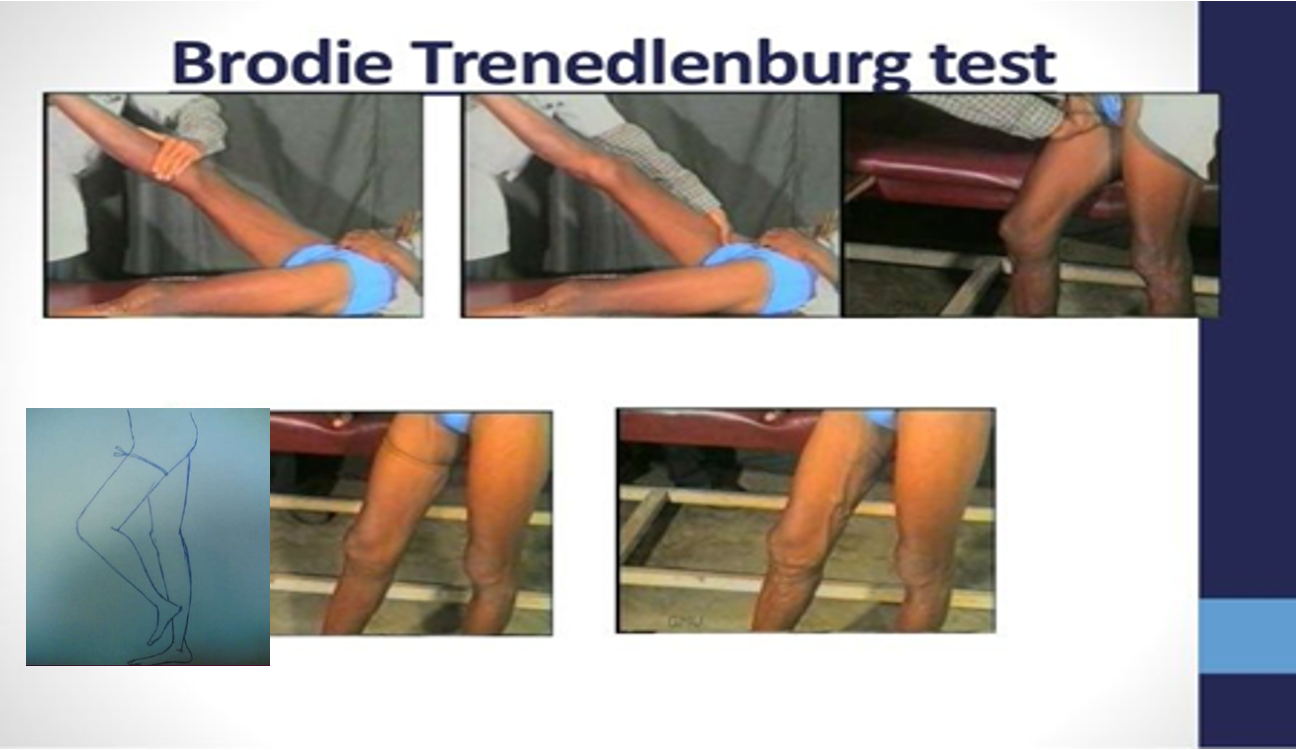
Brodie Trendelenburg test
- Patient’s leg elevated to drain venous blood.
- An elastic tourniquet applied at the sapheno-femoral junction
- The patient then stands with tourniquet in place.
- Rapid filling (<30 seconds) of the great saphenous system- perforator valve incompetent.
- No filling - perforators are competent z
- Now release the tourniquet
- Filling of the great saphenous system from above- sapheno-femoral valve is also incompetent.
Multiple Tourniquet – Triple Test

Auscultation
- Over large veins- murmur in arterio-venous fistula ( veins do not collapse on lying down and can feel pulsation and thrill during palpation)

Daflon tab 500 mgVenotonic