Fistula in Ano
Abnormal chronic tract or cavity that is lined with granulation tissue
Connects a primary opening inside the anal canal to a secondary opening in the perianal skin
Secondary tracts may be multiple and can extend from the same primary opening.
-
Most as result of cryptoglandular infection, & abscess.
-
Low vs High located
-
Symptoms range from minor discomfort and discharge with resultant hygienic problems to sepsis.
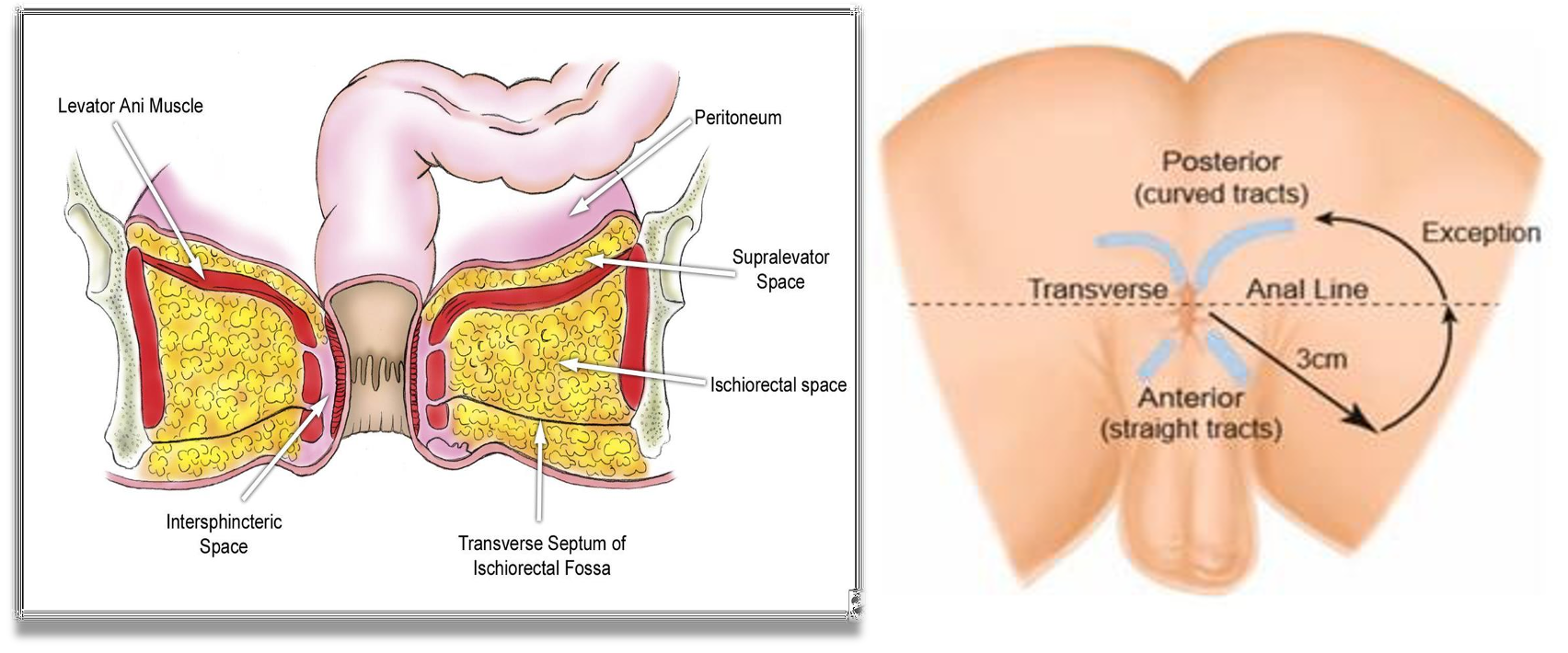
Goodsall’s rule:
Help to identify the anatomy
- Fistulas with an external opening anterior to a plane passing transversely through the center of the anus will follow a straight radial course to the dentate line.
- Fistulas with external openings posterior to this line will follow a curved course to the posterior midline (horseshoe)
Exceptions to Goodsall rule:
- External openings lying more than 3 cm from the anal verge.
- These almost always originate as a primary or secondary tract from the posterior midline, consistent with a previous horseshoe abscess
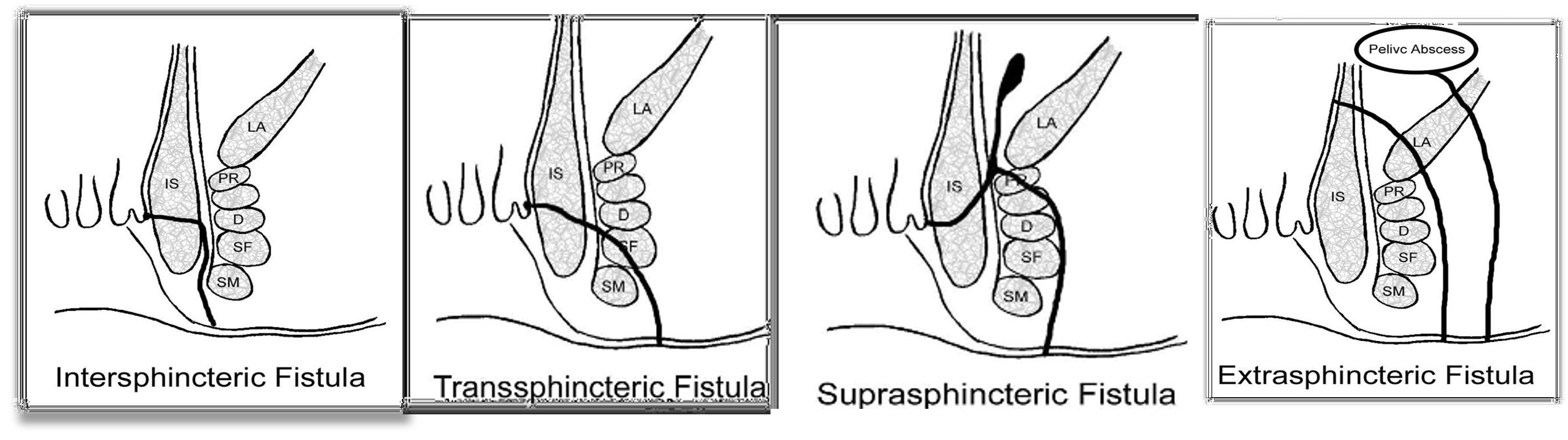
The classification system developed by Parks, Gordon, and Hardcastle Parks classification) is the one most commonly used
It defines 4 types of fistula-in-Ano as follow
| Type of Anal Fistula | Origin | Pathway |
|---|---|---|
| Intersphincteric (70%) | Perianal abscess | Between internal and external sphincter |
| Transsphincteric | Ischiorectal fossa abscess | Into the ischiorectal fossa |
| Suprasphincteric | Supralevator abscess | Tracks superiorly to above the puborectalis |
| Extrasphincteric | Foreign body penetration of the rectum, penetrating injury to the perineum, Crohn disease, Cancer, pelvic inflammatory disease | Tracking upward and through the levator ani muscles to the rectal wall, completely outside the sphincter mechanism |
 |
Patients often provide a reliable history of previous pain, swelling, and spontaneous or planned surgical drainage of an anorectal abscess. Signs and symptoms of fistula-in-ano, in order of prevalence, include the following:
- Perianal discharge
- Pain
- Swelling
- Bleeding
- Diarrhea
- Skin excoriation
- External opening
Physical findings are the mainstay of diagnosis
- Digital rectal examination (DRE) may reveal a fibrous tract or cord beneath the skin
- Discharging perianal sinus
Radiology:
- Fistulography
- Endoanal or endorectal ultrasonography
- MRI
- Others: Scopes-
Management
Treat abscess first (Unless the fistula is superficial and the tract is obvious)
- Fistulotomy vs fistulectomy (+ EUA)
- One stage vs staged procedure (high level ano fistula)
- Seton placement
- Plugs and Adhesives
- Ligation of the intersphincteric fistula tract (LIFT) Procedure:
- A sphincter-sparing procedure for complex transsphincteric fistulas
