- Cranial nerve ex or Rheumatoid ex
- chest pain history
- chest auscultation ( they will ask about Differential diagnosis)
- Lumbar puncture ( ask only Qs no procedure )
- MI counciling
Hx Taking Method
1) Demographic
Name, age, Martial status, Nationality, Residency,
(Occupation also can be said in social history)
EX: 54 year old male driver, not married, lives in apartment in riyadh
2) Chief of complaint
why did you come to hospital; write same as “Abdominal pain ((not specific to Epigastric pain))
3) HPI
- HPI features⇒
- associated symptoms + days + detail, then with exclusion + leg swelling
- B symptoms; weight loss, loss of apetite, fever, night sweats
- then lastly systemic review (could be after past hx)
Complaining of 5 day hx of progressive diffused abdominal pain relieved by sitting, exacerbated by movement associated with… no reported b symptoms… no other system findings…
in depth Systemic review always yes or no question - direct questions
CNS Sys
- ICP; Symptomps
- Motor weakness
- Sensory; parathesia in DM, hemiparesis
- CNV; ask on all cranial nerve symptoms
- Cerebellar; Abnormal movement
- Sphincter; Bladder - autonomic; DM CNS
Cardiac Sys
- Ischemic; Retrosternal pain, Stabbing/Heaving, Radiation proximity, increased with exertion, relieved with glycerine; coronary heart disease; MI, Angina etc…
- Non-Ischemic; Diffused chest pain, increased with cough, strain, breathing; skin infection neuralgia, muscle myopathy, rib fracture/truama costrochondritis, pleural effusion, parynchemous lung, Pulmonary Embolism, SOB
- Grade of dyspnea I-IV; association w/ orthopnea? pillow? wake up w/ SOB? ; paroxysmal
- CVS cause dyspnea; pericarditis, myocardial infarction, valvular heart disease
- RESP cause dyspnea; pneumonia, TB, initial lung fibrosis, cough, Hemoptysis, use of accessory muscles
Resp Sys
- Productive; Phelgm / Nonproductive;Dry - amount, Color, Smell
- Asthma, COPD, Bronchiestasis,
- hemoptysis; resp | Hematemesis; git - frequency, clotting
- bleeding tendency, severe mitral stenosis
GIT Sys
Upper: Heart burn, neusea, vomitting, abdominal pain, dysphagia
- Dysphagia; timing of swallow - oropharyngeal vs esophageal | liquid or solid on dysphagia | Continuous or interrupted | Presentation of: scleroderma, malignancy, Infection, Neusea, vomitting, heart burn, epigastric pain; left
- Pain Radiation
Heaving/ Colicky pain: ?
Radiation epigastric to right shoulder: cholecystitis
Epigastric to back: Pancreatitis
Relieved by leaning forward: pericarditis
- Melena; dark stool if upper GIT blood
- Renal Symptoms: Pyelonephritis, renal stone w/ fever, bone ache, lost of apetite ||| lower with frequency/urgency/like tea?
Lower: ??? CC
itching; obstructive jaundice,
urine, stool, vomitting, loss of weight, job, iv, sexual, fever
autimmune = thallassemia, hemolytic anemia
infectious= malaria
paracetamol liver toxicity - 5 times per day
old age; pancreatic cancer
Gym; anabolic steroid - cholecstsyic jaundice
MSK
-
Joint pain;
- Arthritis; redness, Hotness, swelling, tenderness, limited motility
- Arthralgia;
-
Mechanical vs Inflammatory
- Mechanical; Traumatic - constant bone ache, increased with activity
- Inflammatory; morning stiffness improving with activity
-
Type of Joint
small joint of hand -
Large joint - -
Symmetry
-
Associated Rheuma Symptomps
Autoimmune, SLE, Rheumatoid Arthritis, Lupus
4) Past HX
past medical:
- similar episode as before - (you can mention with HPI)
- Chronic diseases + Family Hx / similar conditions
- Past Admission + transfusion + Surgeries
- Pregnancy / Lactation
- Medication (name dose side effects)
- Allergy
Social: im going to ask some specific question to reach to diagnosis, may i?
- Occupation, Travel, kids, smoking, alcohol, drugs, sexual activity
5) Summary
77 yo sudanese male complaining of chest pain for 9 days which was severe compressing radiating to back associated with cough, with no hx of palpitation, syncopal attack - with hx of cabg.
6) Differential, Impression
put three differential for example;
- autoimmune,
- malignancy,
- infection
7) Workup / Investigation
routine; Blood sugar, electrolyte, CBC
Related to System - Spirometry, Bronchoscopy, MRI, CT etc… ANA antibody sle, specific tests - ANTI-TPO; Thyroid
B- Examination
- introduction, explain examination, take consent, wash hands -
- Exposure | position | privacy (important to mention in every exam process)
1- General Appearance
- Conscious and alert
- features
- connected devices
Summary for general Appearance
EX: elderly male with good build lying comfortable to be - connected to cannula - not connected oxygen. (note general exam findings)
EX: young boy morbidly obese, in resp distress connected to oxygen
2- General examination: ask for Vitals - CHECK Leg swelling
dont touch patient until needed
-
Hand: organized explaination from distal to proximal
- distal - nail, feature…
- dorsum - no janeway…
- flip hand - no osler node…
- specific - cardiac, GIT, Resp
- no infection, no swelling, no deformitiy in dorsum
- no palmar erythema:liver cirrhosis, mitral stenosis , rheumatoid arthritis
- No janeway lesion: CVS
- Leukonechia kolionechia
- Clubbing (window test); Hypoxia; angiogenesis many causes— likely resp cvs, congenital heart diseases, malignancy
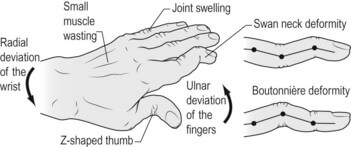
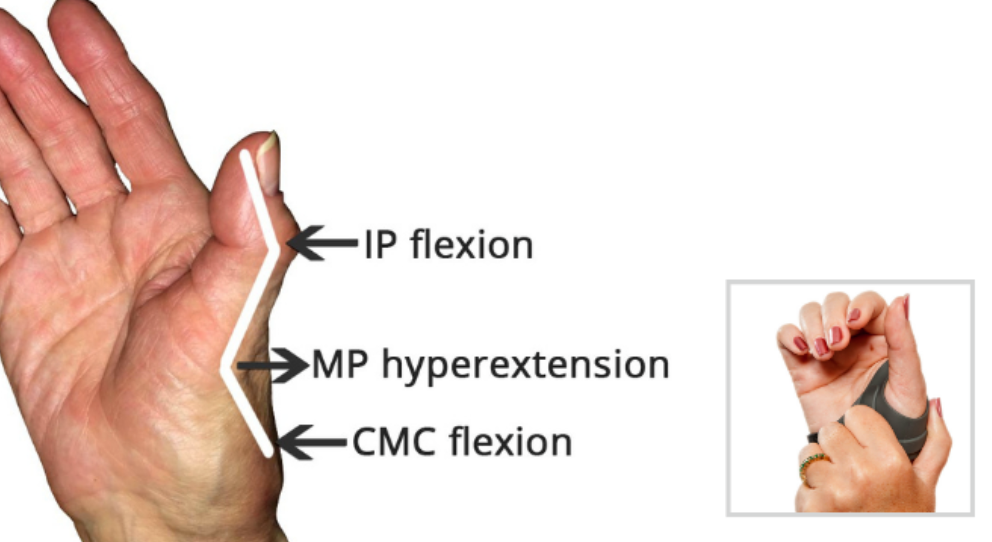
- Rheumatoid deformity w/ ulnar deviation - Z shape thumb, fixed not correctable - ((swan neck vs boutonniere??))
- Sweaty; Hyper
- Thick: Depature contracutre???, hypothyroidism
- Dry: hypo
-
Clubbing - window test
-
Capillary refill
-
Pulse: (rate | rhythm | character | volume | comparison | radioradial delay)
- Dorsalis pedis
- Medial Malleolus
- Popliteal arteria
-
water hammer pulse
-
Vital signs - BP, RR, Temp, Pulse, saturation, - mention need to check
-
Face & Neck: head to neck
- general appearance
- Hair: normal hair distribution
- eye: no pallor/jaundice
- Nasal: no nasal discharge
- Mouth: oral hygiene, central cynosis, oral ulcers
- Neck: no obvious thyroid LN JVP, cyst, swallow - want me to examine?
-
Abdomen: general palpation -
-
Lower Limb: Edema - thumb
Edema Grading- GRADE I: edema from dorsum of foot & then behind medial malleolus bilateral;
- GRADE II: Tibial
- GRADE III: Pinching, catching fold of skin on thigh to check edema
- GRADE IV: Antero-Abdominal wall; peduea orange appearance, thick, red +++ Sacral edema; ascites ((generalized anasarca?))
3- Specific system exam
… revise https://medatlax.com/Clinical/Level-8/Clinical-Medicine/Clinical-Medicine - inspection, palpation, auscultation, percussion
4- thank patient, then document it
5- Summary
old age gentlemen comfortable in bed not in resp distress positive
central cynosis, decrease air entry on right side, lower limb edema
Other notes?
-
Giddiness; sense of blackout when standing up
-
Extrasystole? - af? - irregular ireggularities>
-
leg swelling; edema, SOB; dyspnea
-
smell sputum abcess foul, productive
-
Severe mitral stenosis might present with hemoptysis
-
Aortic Regurge collapsing pulse/ nodding sign
- anemia, paggets disease, pregnancy, thyrotoxicos
- av shunt
-
MCV type of anemia?
-
Platelet count thrombocytopenia; skin rash bleeding tendency
-
ITP, Heparin induced, SLE, Von wil dis, TTP
-
check edema
-
Grades of edema
-
causes of unilateral
-
causes of bilateral: renal, liver, heart…
-
infection, malignancy, autoimmune
-
ROutine Labs - signs each cbc
Chest Pain Hx Case
from CCTD 2 https://www.youtube.com/watch?v=9om2tedf9oo
Station 1
Case scenario summary: + Demographics Yaser is a 65-year-old diabetic and hypertensive ethiopian man works as accountant; minimal movement in work, married.
Chief of complaint: Severe Chest Pain He presented with severe chest pain after lifting up box
HPI Sudden Diffused heavy chest pain with no radiation associated with palpitation no cough, dizziness, nausea, vomitting - the symptom usually came for 45 minutes then subsided in recent episode chest pain persisted until the ER - at rest the pain subsided on lifting of heavy objects the pain exacerbates severity of 6
Past HX i want to ask you personal questions, would help me alot in diagnosis, are you okay with that? known case of HTN First time having chest pain with family hx of DM, MI - previously close relative died from MI
Currently taking medications of nsaids to manage the pain with no known allergen no previous transfusions or surgeries
Yaser works in office, smokes for 10 years - 2 packs a day, drinks alcohol twice or once week, no use of recreational drug use, no previous travel hx
Systemic Review: no headache, no blurred vision no nasal discharge no sore trhoat usual chest pain no constipation diarrhea no abdominal or blood in stool pass medium no blood in urine no skin rashes, eczema good sleep pattern no stress not to cold hot
Guide Case
Student instruction:*
- Obtain an accurate, focused medical history.
- Critically analyze clinical data obtained through history.
- Formulate and prioritize a differential diagnosis using reasoning skills
- Suggest a workup plan
- please take a focused history from this patient.
Presentation of chest pain: Musculoskeletal: costochondrities; worsens with movement, including deep breaths, coughing, and stretching, raising arm skin: Herpes zoster lung: pleuritic pain (sudden and intense sharp, stabbing, or burning pain in the chest when inhaling and exhaling) heart:
-
Acute pain due ACD: angina (come & go // exertion) + MI (At rest)
- protective factor estrogen in females
- II III AVF corresponding leads to inferior wall (specific not widespread)
-
Pericarditis: Acute not severe as angina - mostly viral pericarditis no radiation relieved by leaning forward - supine is worse -
- St Elevation - widespread (rarely could be localized due viral)
-
Fever
esophagus:
esophageal spasm or reflux
Aorta:
- Aortic Dissection: acutely very sharp pain, uncontrolled BP
Chief of Complaint: Severe Chest Pain
HPI S: Site - Retrosternal O: Sudden or gradual | timing C: Stab | Dull | Pricking R: radiation A: angina - palpitation, SOB, Sweating, Dizziness, Syncop, Neusea T: started month ago? do you get it every day? E: alleviated by rest, on elevating on exertion S: Severity - scale of 1 to 10
Past Hx
- Comorbidities any kidney problem?
- Family Hx - anyone in family suffers from …
Systemic Review …
Reference: 1. Talley NJ. Clinical Examination: A Systematic Guide to Physical Diagnosis. 8th ed. New York: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2018. Page: 88, 59-63
2. Kumar P, Clark M. Clinical Medicine. 10th ed. Philadelphia, PA: Elsevier; 2021. 1020, 1028-1029.
3. Lytvyn, Y. et al. (2022) Toronto notes 2022: Comprehensive medical reference and a review for the Medical Council of Canada Qualifying Exam (MCCQE). Toronto, Ontario, Canada: Toronto Notes for Medical Students, Inc. Page : C4-7 Cardiology
Examination
A- Cranial Nerve Examination
5th 7th 8th most commonly appears in exam
https://www.youtube.com/watch?v=yZ5kV7dJoZw
Cranial Nerves
Introduce your self, wash hands, explain the procedures, take consent, assure privacy, position and exposure
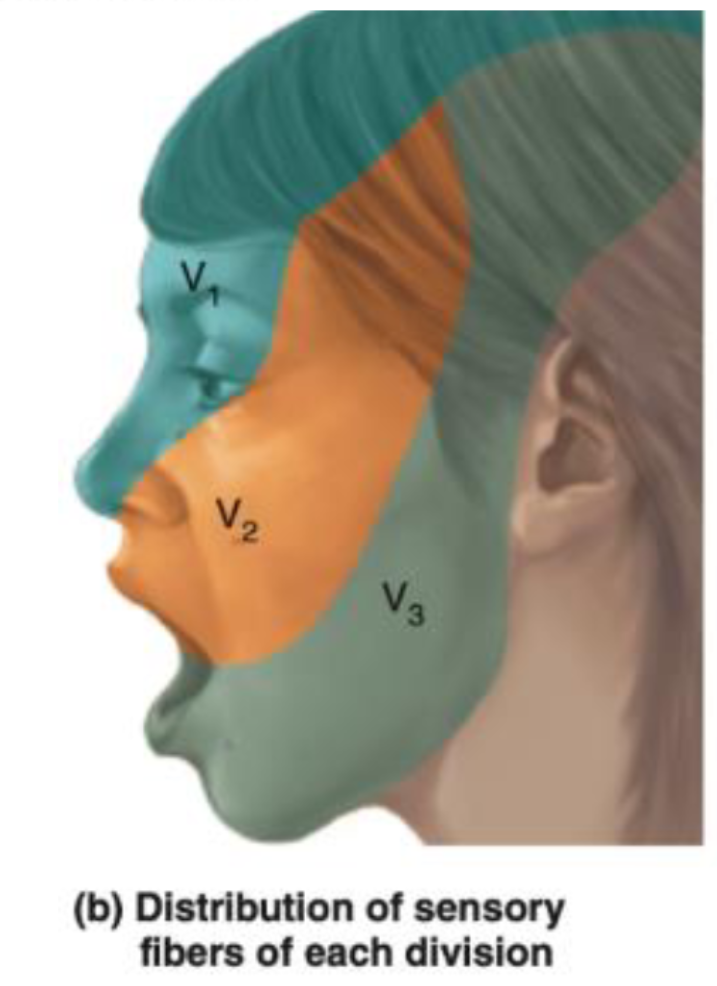
CN V – Trigeminal Nerve
-
Ophthalmic (V1) - Passes through the superior orbital fissure.
- Supplies: Sensation to the forehead, upper eyelid, and cornea.
- Involved in the corneal reflex: The afferent limb (sensory input) of the corneal reflex is through the ophthalmic branch of the trigeminal nerve. The efferent limb (motor output, which closes the eye) is via the facial nerve (CN VII).
-
Maxillary (V2) - Passes through the foramen rotundum.
- Supplies: Sensation to the middle part of the face, cheek, upper lip, and upper teeth.
-
Mandibular (V3) - Passes through the foramen ovale.
- Supplies: Sensation to the lower part of the face, lower lip, and lower teeth. It also carries motor fibers to the muscles of mastication.
- The anterior two-thirds of the tongue receives general sensation (not taste) via the lingual nerve, a branch of the mandibular division.
- Taste from the anterior two-thirds of the tongue is carried by the chorda tympani nerve (a branch of the facial nerve, CN VII), not the trigeminal nerve.
Examination process
-
Sensory Testing:
- Cotton Test: Use a soft piece of cotton to lightly touch different areas of the face. This tests the sensory function of all three branches of the trigeminal nerve. The patient should have their eyes closed during the test to rely solely on their sensory perception. Specifically, test:
- The forehead, upper eyelids, and cornea (ophthalmic branch).
- The cheeks, upper jaw, and upper teeth (maxillary branch).
- The lower jaw, lower teeth, and part of the tongue for general sensation (mandibular branch).
- Cotton Test: Use a soft piece of cotton to lightly touch different areas of the face. This tests the sensory function of all three branches of the trigeminal nerve. The patient should have their eyes closed during the test to rely solely on their sensory perception. Specifically, test:
-
Motor Testing: power (Medial and Lateral pterygoid, temporalis, masseter)
- Mandibular Movements:
- Ask the patient to clench their jaw to test the muscles of mastication, assessing the motor function of the mandibular branch (V3).
- Have the patient open their mouth and then move their jaw side to side, observing for any deviations or difficulties, which might indicate an issue with trigeminal motor function or asymmetrical muscle weakness.
- Mandibular Movements:
buccinator supplied by facial
-
Reflex: Jaw Reflex (afferent efferent) - Pure reflex Gently tap the jaw with the mouth slightly open to check the reflex. A normal response would be a slight and quick involuntary clenching of the jaw. An exaggerated response might suggest abnormalities in the reflex arc, which is primarily controlled by the sensory and motor roots of the mandibular branch.
Corneal reflex (Afferent Opthalmic - efferent by facial)
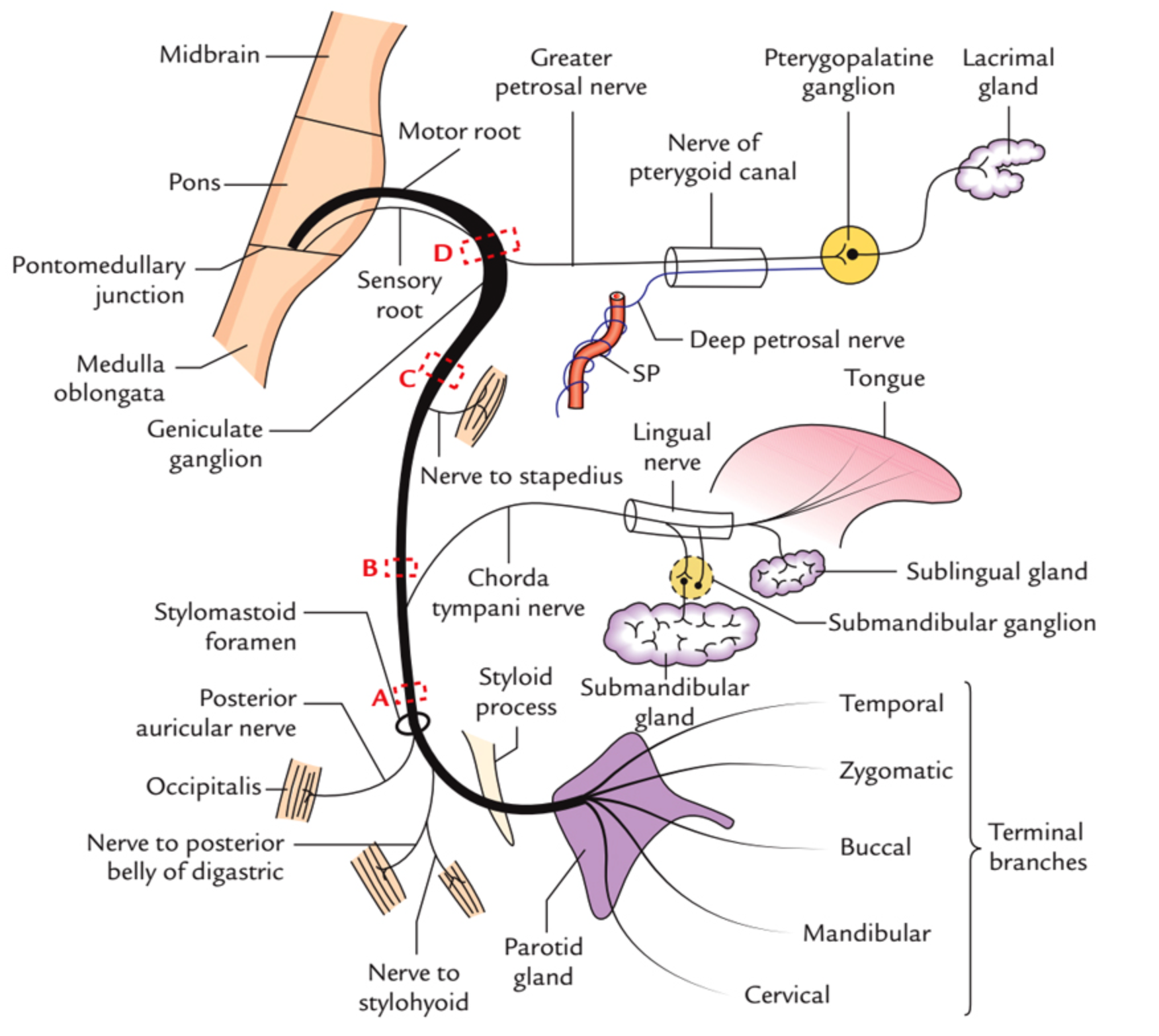
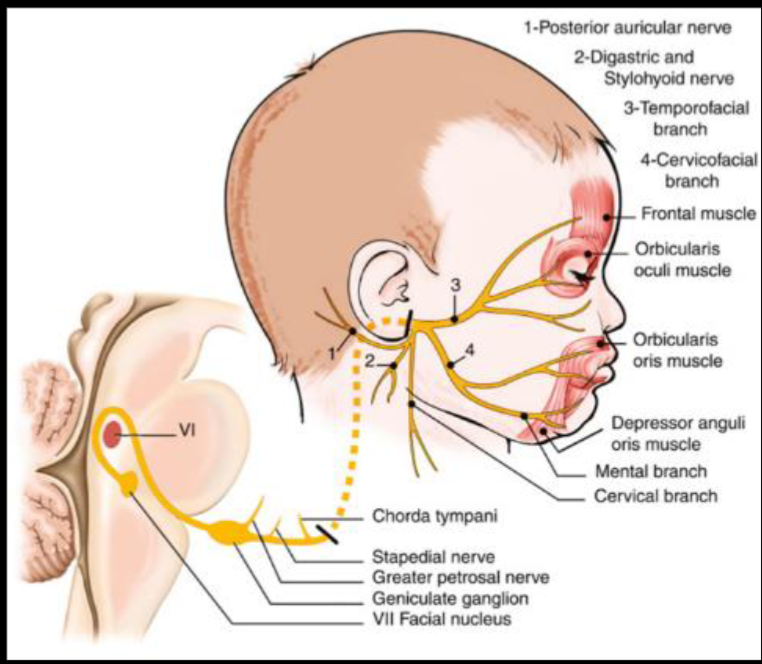
CN VII - Facial Nerve
 Course???
Course???
in middle ear gives two branches to chorda tympani & Stapedius (ear distrubance)
Innervations - External acoustic meatus - for sensation of ear - Motor - Movement of the face - Sternomastoid - branches nerve to stapedius - Loud sounds middle ear - & nerve to chorda tympani - Parasympathatic Submandibular & Sublingual gland
Tests
- Temporalis - raise eye brows (dont use hands )
- Orbicularis Oculi - check for resistance when eyes close
- Buccinator - Blow (palpate)
- Levator Anguli Superioris - smile
- Orbicularis Oris - whistle
- Taste anterior 2/3
 UMN Palsy - Causes Includes; (hyperreflexia)
- stroke
- MS
- trumours
- Internal capsule palsy
- Eyebrow raise is normal - if botox, contraindicated for the test
UMN Palsy - Causes Includes; (hyperreflexia)
- stroke
- MS
- trumours
- Internal capsule palsy
- Eyebrow raise is normal - if botox, contraindicated for the test
LMN Palsy - Causes includes
- Bells palsy
- Cavernous sinus thrombosis
- Fracture (truama) base of skull
- Acoustic neuroma
- Shingles
- Ramsay Hunt Syndrome with skin lesioned shingles on face and ear due to varicella ,
- Eyebrow doesn’t raise compared to contra-lateral
Bilateral facial nerve palsy - Sarcoidosis - Guillain-Barré Syndrome - Lyme disease due internal capsule
other notes botox mask symptoms of UMNL of facial nerve
most common causes of stroke? DVT - Stroke may transfer DVT to brain ASD - ventricular - patent foramin ovale
CN VIII - Vestibulocochlear
internal acoustic meatus enters to the skull depolization through potassium -
Cochlear division;
-
Whisper on ear while other is closed - tell him to repeat to confirm.
-
Rinne Test:
- This test compares air conduction to bone conduction. A tuning fork is used initially to assess bone conduction by placing it on the mastoid process. It is then held near the ear canal to assess air conduction.
- A positive Rinne test (air conduction is better than bone conduction) indicates normal hearing or sensorineural hearing loss.
- A negative Rinne test (bone conduction is better than or equal to air conduction) suggests conductive hearing loss.
-
Weber Test:
- This test assesses bone conduction using a tuning fork, which is placed on the center of the forehead.
- The purpose is to determine the lateralization of sound. Sound lateralization to one ear typically indicates sensorineural hearing loss in the opposite ear or conductive hearing loss in the ear to which sound is lateralized.
sensorineural causes - Neurofibromatosis type 2 - Noise pollution - Aminoglycosiedes - Gentamycin - Test, with ringing on frontal head - check for which ear hears most = laterilzation of normal side - Pendred Syndrome = Goiter + hearing loss (thyroid manifestations are rare, but may be presentaiton)
Conductive deafness - Wax / foreign objects - Otitis Media - - Tympanic membrane rupture - Otosclerosis. - Swimmers ear - Foreign body
Note
Fracture at the base of the skull can cause sensorineural hearing loss and bleeding, with lateralization. This is a result of conductive deafness, as the vestibulocochlear nerve passes through the petrous part of the temporal bone.
B- Rheumatoid Arthritis Examination
https://www.youtube.com/watch?v=GhQVp_xdGVA
Scenario: A young female patient presents with symptoms suggestive of Rheumatoid Arthritis (RA).
- Anti-TNF-α: Infliximab (screen for latent TB and opportunistic infections before starting; consider interferon-gamma release assay). Adalimumab is another anti-TNF agent.
- Anti-IL1: Other agents in this group include anakinra, canakinumab, and rilonacept.
Notes:
- Rifampicin can cause discoloration and affects RNA synthesis.
- Jones criteria are used for the diagnosis of rheumatic fever, not RA.
Investigations
- Complete Blood Count (CBC)
- Erythrocyte Sedimentation Rate (ESR)
- C-Reactive Protein (CRP)
- Joint X-ray
Pathophysiology (5 points)
- Synovial inflammation and proliferation
- Soft tissue swelling
- Narrowing of joint spaces
- Bone erosion
- Deformity and functional impairment
Characteristic Features:
- Migratory polyarthritis
- Primarily affects small joints of the hands, especially the proximal interphalangeal (PIP) joints, but spares the distal interphalangeal (DIP) joints.
- Rheumatoid factor (RF) is often positive but may be negative in early disease.
Differential Diagnosis
- Psoriatic arthritis (may precede skin manifestations by 10 years; differentiate with X-ray)
- Systemic Lupus Erythematosus (SLE)
- Reactive arthritis (formerly known as Reiter’s syndrome; often follows an infection)
- Osteoarthritis (more common in older individuals; can occur in younger individuals with repetitive joint use, e.g., piano players)
Initial Management
- Nonsteroidal anti-inflammatory drugs (NSAIDs)
- Corticosteroids (oral or intra-articular injections to control flares)
Approach to Examination
introduce your self, explain the procedure, take consent, wash hands, assure privacy, position and exposure make sure to remove clothing, avoid snake stethoscope
- Be mindful of patient comfort: Offer a pillow for support and avoid shaking hands if the patient is experiencing joint pain.
- Mnemonic (DAF):
- Deformity: Inspect the hands systematically, moving from medial to lateral and distal to proximal.
- Ulnar deviation
- Swan neck deformity (hyperextension of PIP joint, flexion of DIP joint)
- Boutonniere deformity (flexion of PIP joint, extension of DIP joint)
- Z deformity of the thumb
- Guttering (loss of muscle bulk between metacarpals, tendor clear)
- Palmar erythema; Thenar eminence atrophy
- Scars from previous surgeries or joint injections
- Rheumatoid nodules
- psoriatic rash same as RA (behind ear, and elbow)
- Activity: Assess disease activity (e.g., presence of flares, joint tenderness, swelling, warmth, tighness). four t’s and one s -
- Gently palpate the joints for tenderness,
- swelling (RING TEST),
- tapping; parathesia around distribution of hand (induce pain, never do in exam) (do you feel pain when you tap here before?)
- warmth/temp (from forearm, distal, forarm, phalanges.), avoid affected joints
- tightness pinch test if patient has frequent flares we give steroids will break down collagen/ellastin - become like paper ++ cushing - sometimes skin is tight glued to the skin - systemic scleroderma - mixed connective tissue disease
- Function of hand: Evaluate hand function (e.g., grip strength, ability to perform fine motor tasks). - special tests
- Thumb opposition: Ask the patient to touch the tip of their thumb to the tip of each finger. Z TASBEEH
- OK SIGN median nerve compensation
- COIN TEST; pencil grip - abnormal with compensation due deformities
- Phalen’s test and Tinel’s sign: to assess carpal tunnel syndrome (median nerve compression) dorsum to dorsum dorsal to dorsal arm - results in parathesia - dont do it if he has this previous symptom
- Deformity: Inspect the hands systematically, moving from medial to lateral and distal to proximal.
Systemic Examination
-
General inspection: Look for signs of:
-
Jaundice (scleral icterus)
-
Pallor (conjunctivae); due Anemia, hemolytic anemia, methotrexate folate defieciency; megaloblastic anemia
-
Butterfly rash (malar rash characteristic of SLE)
-
Round face (Cushing’s syndrome) - interscapular cushing pad, previous surgery scar atlantoaxial subluxation (spastic paraperesis in lower limb) - Ask patient consent before going his back for interscapular pad of fat for cushing
-
Smooth tongue (iron deficiency anemia or oral candidiasis; inhaled corticosteroids)
-
Peripheral edema (pitting edema in the lower extremities)
-
-
Cardiovascular: Auscultate for murmurs and signs of pulmonary hypertension (e.g., loud P2).
-
Respiratory: Auscultate the lungs for crepitations/Fine Crackles (suggestive of interstitial lung disease).
-
Gastrointestinal: Palpate the abdomen for hepatomegaly (liver enlargement).
-
Musculoskeletal: Examine other joints for signs of arthritis (e.g., knees, ankles).
Potential Complications and Considerations in General Examination findings
- Anemia: Can be caused by iron deficiency (due to gastrointestinal blood loss from NSAID use), chronic disease, or autoimmune hemolytic anemia (Jaundice * & Methotrexate & Autoimmune hepatitis due nature of autoimmunity) - could be also due gastric ulceration loss of blood +++ B12 deficiency anemia; depleted folate
- Methotrexate toxicity: Monitor liver function tests and complete blood counts.
- Infection: Increased risk due to immunosuppressive medications.
- Scleritis and episcleritis: Inflammation of the eye.
- Cushing’s syndrome: Due to prolonged corticosteroid use resulting in PROXIMAL MYOPATHY.
- Osteoporosis: Due to chronic inflammation and corticosteroid use.
- Cardiovascular disease: Increased risk in patients with RA.
- Amyloidosis: Can lead to nephrotic syndrome.
- Analgesic nephropathy: Chronic kidney disease due to long-term NSAID use.
fletus syndrome; development of spleenomegaly due RA - destroyed RBCs resulting Anemia
Further Investigations (if indicated)
- Renal function tests
- Liver function tests
- Serum creatinine
- Urinalysis
- Chest X-ray (Multiple nodules in periphery of the lung - looks like rheumatoid - bilateral homogenous circumscribed nodules; most like pneuomocoisosis; coal worker; caplan syndrome, and RA)
- Echocardiogram
Examination findings of a Patient Potentially with Rheumatoid Arthritis and Complications
Cardiovascular:
- 2nd LT ICS - Loud S2: This finding suggests pulmonary hypertension. Pulmonary hypertension can be a primary condition or secondary to another underlying issue, such as interstitial lung disease (a potential complication of rheumatoid arthritis).
- Right sided HF = pulmonary HTN - Edema - associated with Hepatomegaly (Methotrexate)
Abdomen:
- Hepatomegaly: Enlarged liver. Several potential causes are listed, reflecting the complexity of this patient’s case:
- Methotrexate: A common medication for RA, it can cause liver toxicity.
- Right-sided Heart Failure: Pulmonary hypertension can lead to right-sided heart failure, causing congestion in the liver.
- Autoimmune Hepatitis: RA is an autoimmune disease, and other autoimmune conditions, like autoimmune hepatitis, can co-occur.
Fever:
- Azathioprine-induced Neutropenia: Azathioprine, another immunosuppressant used in RA treatment, can cause neutropenia (low neutrophil count), increasing the risk of infection and fever.
Felty’s Syndrome:
- Splenomegaly, Pancytopenia, Pallor: Felty’s syndrome is a rare complication of long-standing RA characterized by an enlarged spleen, decreased red blood cells, neutrophils, and platelets. The reduced red blood cell count can result in pallor, which might be visible on eye examination.
Renal:
- Amyloidosis: Amyloidosis is a rare but serious complication of chronic inflammatory diseases like RA. It can lead to nephrotic syndrome, characterized by proteinuria and edema. Ballottement of the kidney may be a sign of an enlarged kidney due to amyloid deposits.
- NSAID-induced Nephropathy: Long-term use of NSAIDs for pain relief can contribute to kidney damage (analgesic nephropathy), especially in patients with pre-existing renal issues.
Musculoskeletal:
- Joint Crepitus (Knee): Crepitus is a grating or crackling sound or sensation in a joint, often associated with arthritis. Further examination, including range of motion assessment (e.g., flexion), is needed.
Lower Limbs:
- Edema: Swelling, likely in the lower extremities, suggesting right-sided heart failure secondary to pulmonary hypertension. + amyloidosis
Endocrine:
-
Suspected Cushing’s Syndrome: The notes suggest concern about possible Cushing’s syndrome, likely due to the patient’s clinical presentation or long-term steroid use for RA.
- Dexamethasone Suppression Test:
-
Low-dose: This is the initial screening test to confirm elevated cortisol levels.
-
High-dose: If the low-dose test is abnormal, a high-dose test can help differentiate between Cushing’s disease (pituitary tumor causing excess ACTH) and other causes of Cushing’s syndrome (e.g., adrenal tumor, ectopic ACTH production).
-
-
24-Hour Urinary Free Cortisol Test
-
Late-Night Salivary Cortisol Test
- Dexamethasone Suppression Test:
-
Differential Diagnosis: The differential diagnosis for elevated cortisol includes Cushing’s syndrome, pseudo-Cushing’s syndrome (often seen in conditions like alcoholism or depression), and exogenous steroid use.
Further Investigations:
This patient requires further investigations to confirm the diagnoses and assess the severity of their conditions. This may include:
- X-ray of joint - most importantly
- Echocardiogram: To assess the severity of pulmonary hypertension and right heart function.
- Pulmonary Function Tests: To evaluate lung function and identify any underlying lung disease.
- Liver Function Tests: To assess liver health and monitor for methotrexate toxicity.
- Kidney Biopsy: To confirm amyloidosis and assess the extent of kidney damage.
- Imaging (e.g., CT/MRI): To evaluate the spleen, liver, kidneys, and adrenal glands.
- Autoantibody Testing: To look for specific autoantibodies associated with autoimmune hepatitis and other autoimmune conditions.
Treatment
DMARDS - corticosteroid as bridging treatment
Disease-Modifying Antirheumatic Drugs (DMARDs)
- Methotrexate
- Azathioprine (Isiosyprine is likely a typo); inhibit synthesis of purine - adverse; neutropenia
- Hydroxychloroquine; adverse; retinal deposits
- Gold compounds; nephrotic, skin pigmentation, encephalitis,
- Leflunomide; pyrimidiine synthesis inhibitor - only treatment for RA - results in tachycardia.
Treatment Strategy:
- Corticosteroids + Methotrexate for 6 months initially. ??? CC
- If acute disease persists, consider adding a biologic agent (e.g., anti-TNF-A (Infliximab & another mab) or anti-IL1).
- If no response to DMARDs, administer biological agents (antibodies, cytokines).
Screen TB before giving ANTI-TNF-A medications
C- Chest auscultation
(differential diagnosis will be asked)
introduce your self, explain the procedure, take consent, wash hands, assure privacy, position and exposure make sure to remove clothing, avoid snake stethoscope
RESP Auscultation
https://youtu.be/gRWSyqatWQQ?t=263
-
To assess breath sounds, ask the patient to breathe in and out slowly and deeply through the mouth.
-
Begin at the apex of each lung and zigzag downward between intercostal spaces. Listen with the diaphragm portion of the stethoscope.
Process
- Using the diaphragm of a stethoscope & comment on the following:
- Breath sounds (BS)
- Intensity: Normal or ↓ as in (consolidation, collapse, pleural effusion, pneumothorax, lung fibrosis)
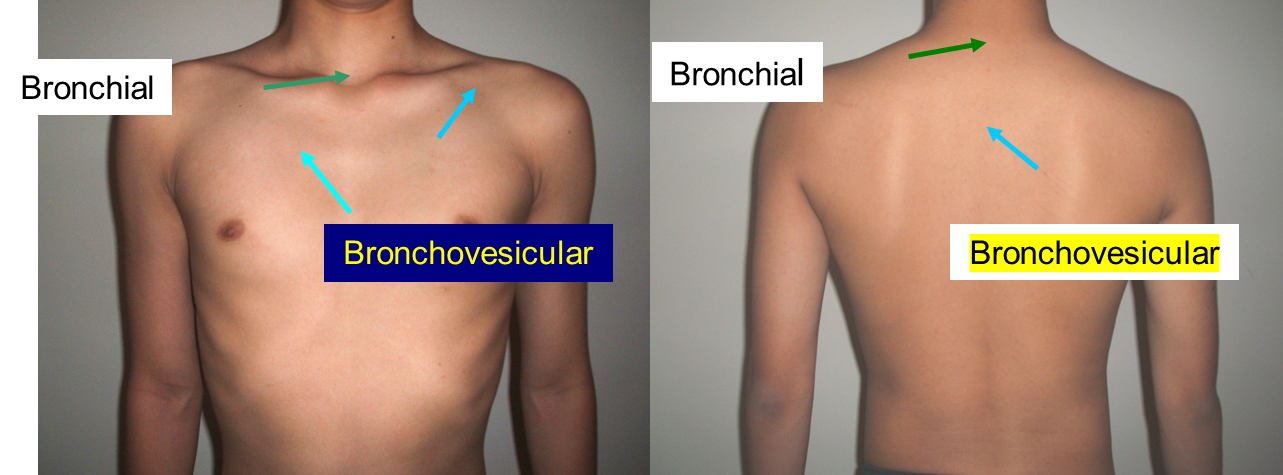
- Quality: Vesicular or bronchial
- Differentiation between vesicular & bronchial
- Vesicular: louder & longer on inspiration & has no gap between the 2 phases
- Bronchial: louder & longer on expiratory & has a gap between the 2 phases
Order of auscultation
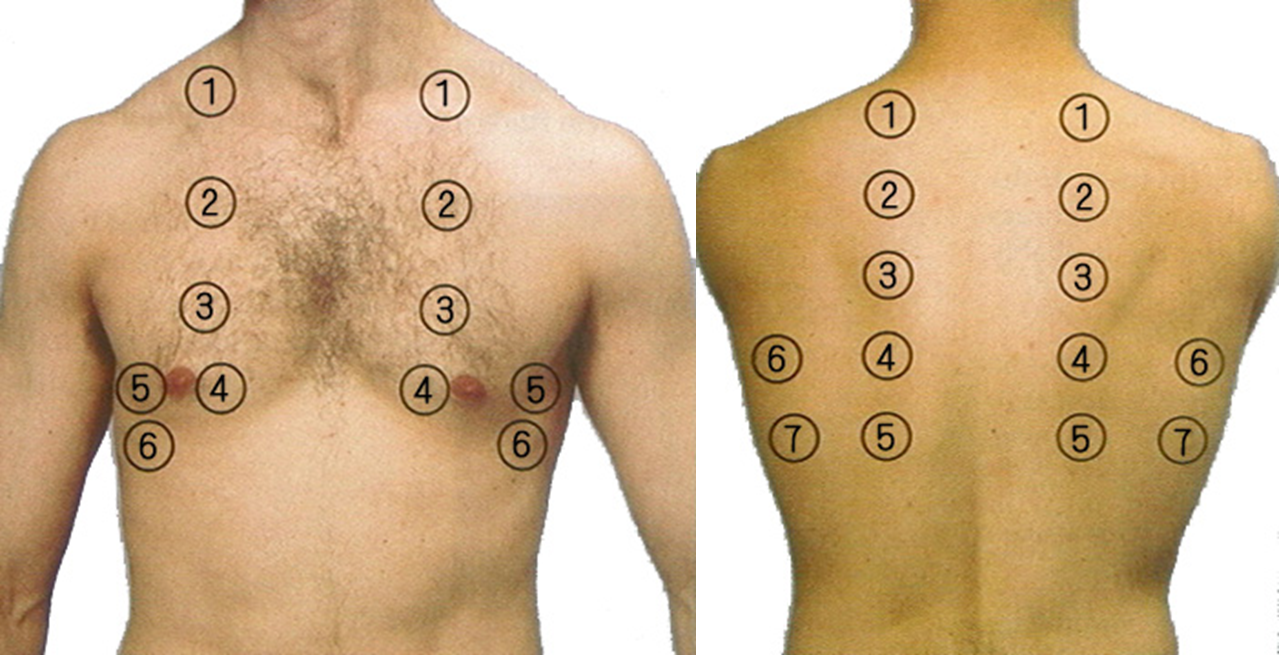
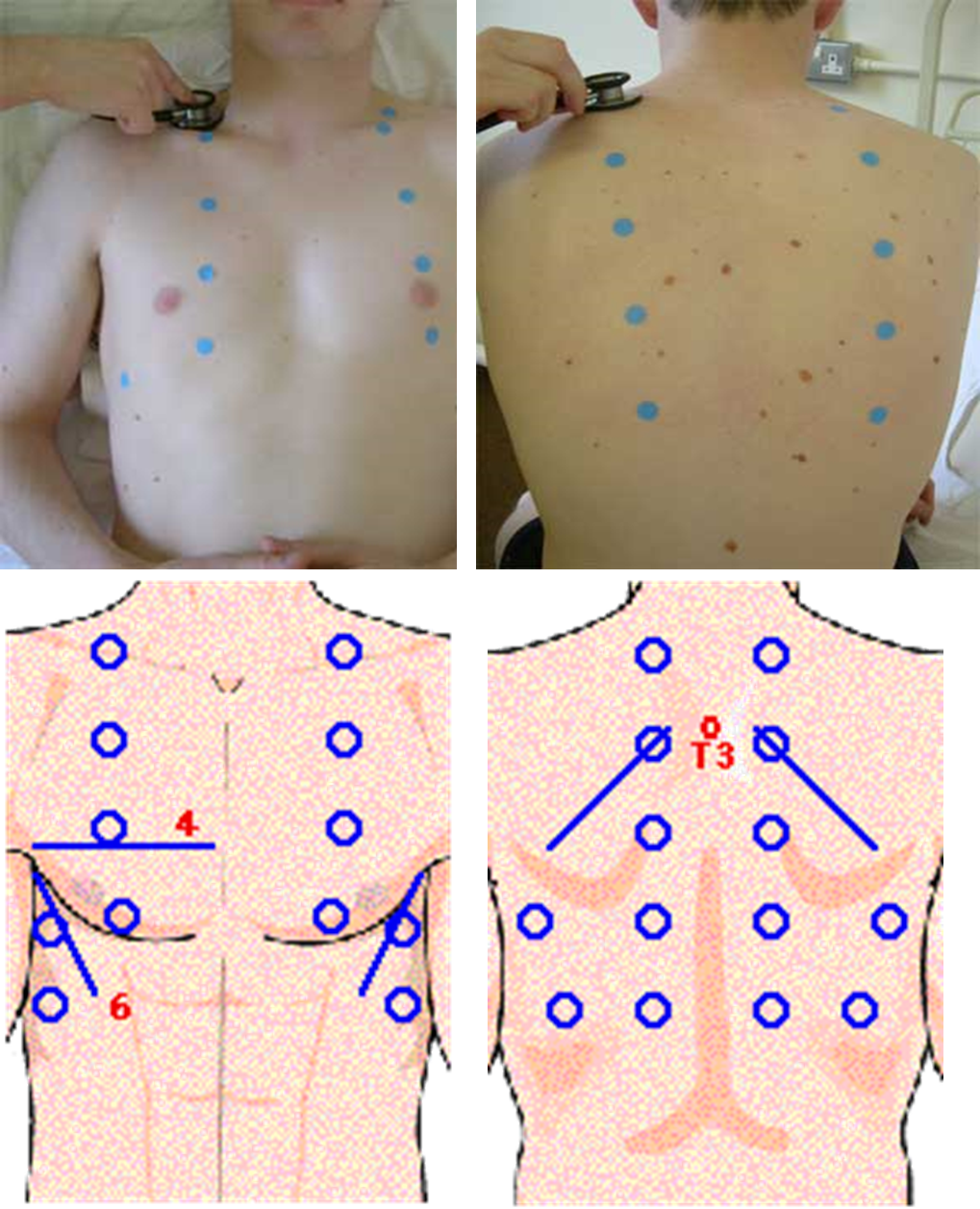
1- Comment on Air Entry
Reduced in lung diseases, pulmonary collapse, pneumothorax
2- Comment on Breath sound
| Sound | Description | Common Causes |
|---|---|---|
| Vesicular (COPD expiration become prolonged in compare with normal). | Soft, low-pitched, normal over most lung fields | Normal lung function |
| Bronchial | Loud, high-pitched, normal over trachea - Larynx, suprasternal fossa, around 6th, 7th cervical vertebra, 1st, 2nd thoracic vertebra | Normal over trachea, abnormal if heard elsewhere |
| Bronchovesicular | Intermediate pitch, normal near sternum/scapulae 1st, 2nd intercostal space beside of sternum, the level of 3rd, 4th thoracic vertebra in interscaplar area, apex of lung | Normal lung function |
| Crackles (Rales) | Discontinuous, popping sounds (fine or coarse) | Pneumonia, heart failure, fibrosis, bronchiectasis |
| Wheezes | Continuous, high-pitched, musical | Asthma, COPD, bronchitis, airway obstruction |
| Rhonchi | Low-pitched, snoring or gurgling | Chronic bronchitis, pneumonia, cystic fibrosis |
| Stridor | High-pitched, harsh, inspiratory sound | Upper airway obstruction (croup, epiglottitis, tumor) |
| Pleural Rub | Creaking or grating sound | Pleuritis, pulmonary embolism, pneumonia |
| Absent/Diminished | Reduced or absent breath sounds | Pneumothorax, pleural effusion, atelectasis |
lastly cover the patient and thank him then wash your hands
Station Procedure Lumbar Puncture
(examiner will ask questions mostly) Lumbar Puncture CSF fluid
Prerequisites
- Obtain a thorough medical history, paying attention to bleeding tendencies, atrial fibrillation, and anticoagulant use (e.g., warfarin).
- Perform a CT scan if a space-occupying lesion (SOL) is suspected.
- Obtain informed consent from the patient.
Contraindications
- Space-Occupying Lesion (SOL): Risk of herniation.
- Bleeding Disorders: Conditions such as hemophilia.
- Anticoagulant Use: Patients on anticoagulants (e.g., warfarin).
- Thrombocytopenia: Low platelet count.
- Vertebral Abscess: Risk of infection.
- Spinal Deformities: Conditions like scoliosis; consider ultrasound guidance.
- Phenytoin Use: Risk of spina bifida.
Diagnostic Indications
- Meningitis: Lumbar puncture is used to diagnose infections like bacterial, viral, or tuberculous meningitis.
- Encephalitis
- Neurosyphilis
- MS , GBS
- Subarachnoid Hemorrhage
- Carcinomatous Meningitis
- Monitoring Hydrocephalus
Other Therapeutic Uses
- Antibiotic Administration
- Anesthesia (e.g., spinal anesthesia)
Complications
- Headache (most common)
- Epidural or subarachnoid hematoma
- Spinal cord trauma
- Infection
- Back pain (most common)
- Hypotension, bradycardia.
Risk Factors
- Papilledema: Risk of blindness due to idiopathic intracranial hypertension if not properly managed.
Position The preferred position is lying on their side (left lateral) with the patient’s legs flexed at the knee and pulled in towards their chest, and upper thorax curved forward in an almost fetal position.
The second position is the upright or sitting position. Sit the patient on the edge of bed, with their legs resting on a stool or chair, ask them to roll their shoulders and upper back forwards and the chair is positioned to bring the thighs up towards the abdomen. Full Procedure introduce yourself, explain procedure, take consent, wear sterile gloves, assure privacy, exposure and position - ready equipment (LP Tray)
-
Feel the pelvis after position - iliac crest will pass by L4 - then trace your fingers downwards by one process for L3. then mark it
-
Start sanitizing the area three times from Inside to outside best circular motion - start centrally then peripherally
-
use sterile paper drape after sanitizing the whole back - centrally to the mark
-
Anesthesia: Apply lidocaine for local anesthesia Inject Subcutaneous (30 degree) anaesthetics (lidocaine) to the area. Avoid lidocaine in patients with liver cirrhosis; consider using ether-based anesthetics in such cases (Isoflurane, desflurane, and sevoflurane)
-
Needle Insertion: with spinal needle Insert the needle between the marked L3-L4 at 15 degree from 90 degree angle until pop is felt. dont pull puncture until its fully secured to prevent complications
-
Sample Collection: Collect 4 samples for:
- Chemistry
- Cytology
- Microbiology
- fourth-fifth just incase for other labs
LP Tray includes
- Spinal needle
- Three-way stopcock
- Manometer
- specimen tubes
- Local anesthesia such as: Xylocaine /lidocaine 1%
- Betadine: (Povidone-iodine) solution & sponge wand.
- Drapes, gauze, and bandage
Note Subarachnoid Hemorrhage: If the sample is red, it may indicate a subarachnoid hemorrhage. - Look for xanthochromia (yellow discoloration) in the CSF also indicates subarachnoid hemorrhage
Post-Procedure Counseling
- Advise the patient to rest on their back and drink coffee to help prevent post-LP headaches.
- If a severe headache occurs, consider performing a blood patch to equalize CSF pressure.
How to minimize the headache?
- choice of needle standerd Quinck versus atraumatic .
- decrease the number of attempts.
- reinsersion of the stylet.
- bed rest after the procedure.
CSF Analysis
| Parameter | Bacterial Meningitis | Tuberculous (TB) Meningitis | Viral (Aseptic) Meningitis |
|---|---|---|---|
| Appearance | Turbid, cloudy | Slightly turbid or clear | Clear |
| Opening Pressure | Elevated (200-500 mm H₂O) | Elevated (200-300 mm H₂O) | Normal or slightly elevated |
| White Blood Cell (WBC) Count | Elevated (1,000-5,000 cells/µL) | Elevated (100-500 cells/µL) | Elevated (10-500 cells/µL) |
| WBC Differential | Predominantly neutrophils (PMNs) | Predominantly lymphocytes | Predominantly lymphocytes |
| Protein | Elevated (100-500 mg/dL) | Elevated (100-300 mg/dL) | Mildly elevated (50-100 mg/dL) |
| Glucose | Decreased (<40 mg/dL or <40% of serum) | Decreased (<45 mg/dL or <40% of serum) | Normal or slightly decreased (>45 mg/dL) |
| CSF/Serum Glucose Ratio | Low (<0.4) | Low (<0.4) | Normal (>0.6) |
| Lactate | Elevated (>3.5 mmol/L) | Elevated (2.5-4 mmol/L) | Normal (<2 mmol/L) |
| Culture | Positive for bacterial pathogens | Positive for Mycobacterium tuberculosis | Negative |
https://medatlax.com/Clinical/Level-8/Skill/Topics/Lumbar-Puncture/Lumbar-Puncture
https://medatlax.com/Clinical/Level-8/Skill/Topics/Lumbar-Puncture/Lumbar-Puncture-Procedure
Station Counseling
https://www.youtube.com/watch?v=cEeX5lkNhk0 https://www.youtube.com/watch?v=UJncSUbBEIU
Case 1: - Post Mi Counseling
introduce your self, what you do, explain about their situation. take Hx necessary for effective counseling
Introduction:
- Begin by discussing the patient’s current situation. Ask if they recall any events or symptoms leading up to the episode. Specifically, inquire if they experienced unconsciousness or any other significant symptoms before the MI.
Diagnosis and Management:
- Explain that the patient has been diagnosed with a myocardial infarction (heart attack) and that appropriate management has been initiated.
- Ask the patient if they understand their diagnosis and provide a brief explanation of the condition, including: - Pathophysiology - Risk factors (e.g., smoking, high blood pressure, high cholesterol, diabetes). - Symptoms (e.g., chest pain, shortness of breath, fatigue). - Protective factors (e.g., lifestyle changes, medications). - Effect of medications (e.g., aspirin, beta-blockers, statins) and how they help prevent future episodes.
History and Lifestyle:
- Take a detailed history, including:
- Medication use (e.g., aspirin).
- Smoking history (e.g., 1 pack per day for 15 years, attempts to quit) suggest smoking cessation clinic
- Exercise
- Travel
- Discuss the importance of lifestyle changes, such as smoking cessation, diet, and exercise.
Activity and Restrictions: Discuss the patient’s ability to return to normal activities, including:
- Driving: No driving for 2 weeks, and if the patient is a large veichle driver, they should avoid driving for 6 weeks.
- Travel: Delay travel for 1 week post-PCI (Percutaneous Coronary Intervention) with stent placement.
- Exercise: Encourage light exercise, such as going to the gym, but advise avoiding excessive strain.
- Sexual activity: abstain for 6 weeks
- Thrombolytic therapy: If applicable, explain that they should avoid strenuous activities for 2 weeks after receiving thrombolytic therapy such as contact sport.
Follow-Up and Monitoring:
-
Schedule follow-up appointments for screening and management of conditions such as diabetes (DM) and hypertension (HTN).
-
Provide written instructions for the patient to refer to later.
-
importance of compliance with medication
-
Symptoms to look out for
Questions and Patient Understanding:
- Throughout the conversation, ensure that the patient understands the information being provided. Establish clear communication and ask if they have any questions on every point you go over
- Reassure the patient that they may need to take time off work (three weeks to one month) and discuss any concerns they may have about their job or recovery.
Conclusion:
-
Provide the patient with a leaflet summarizing the key points discussed, including lifestyle changes, medication instructions, and follow-up care.
-
Ask if they have any final questions or concerns before concluding the session and thank the patient
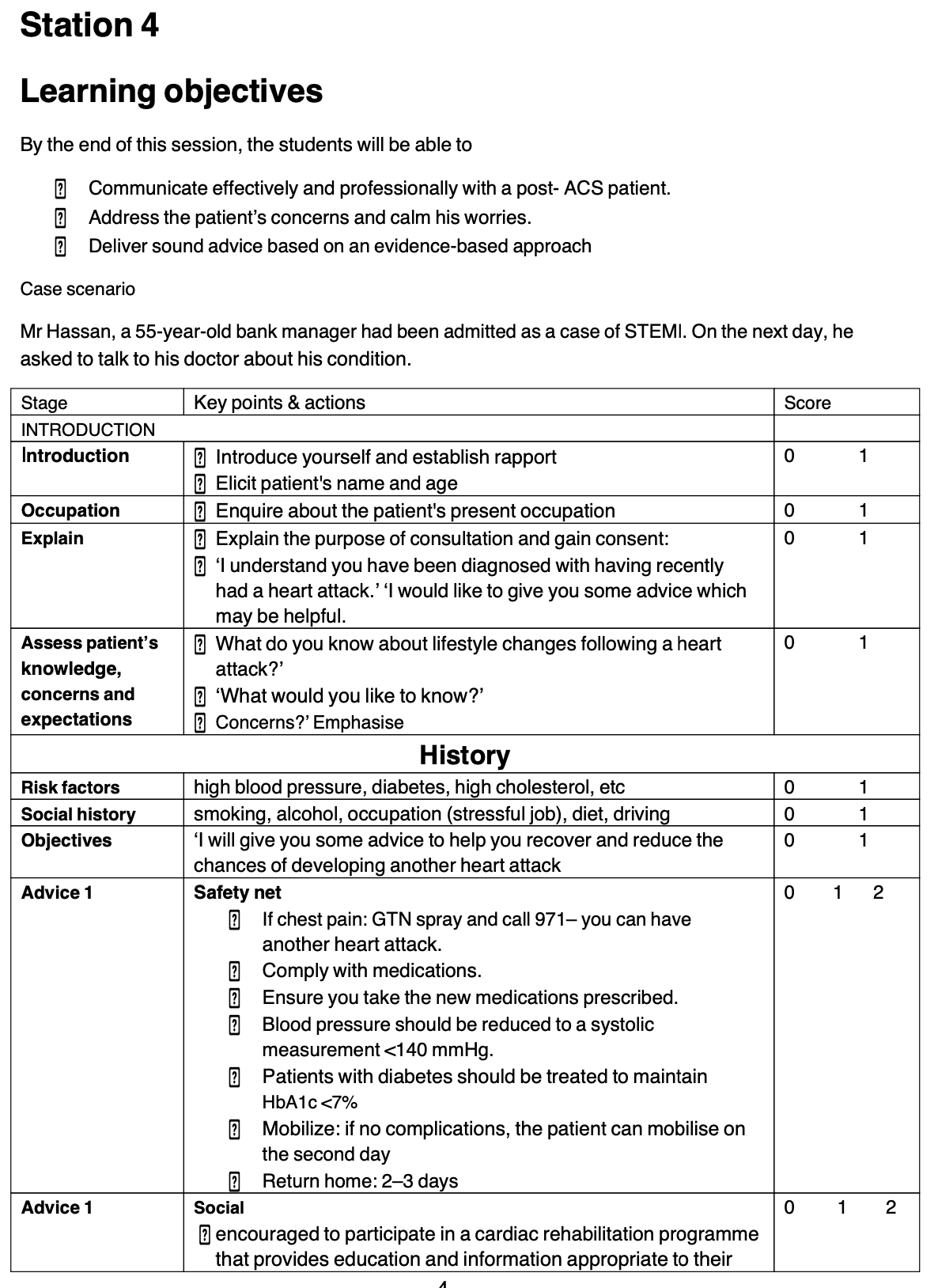
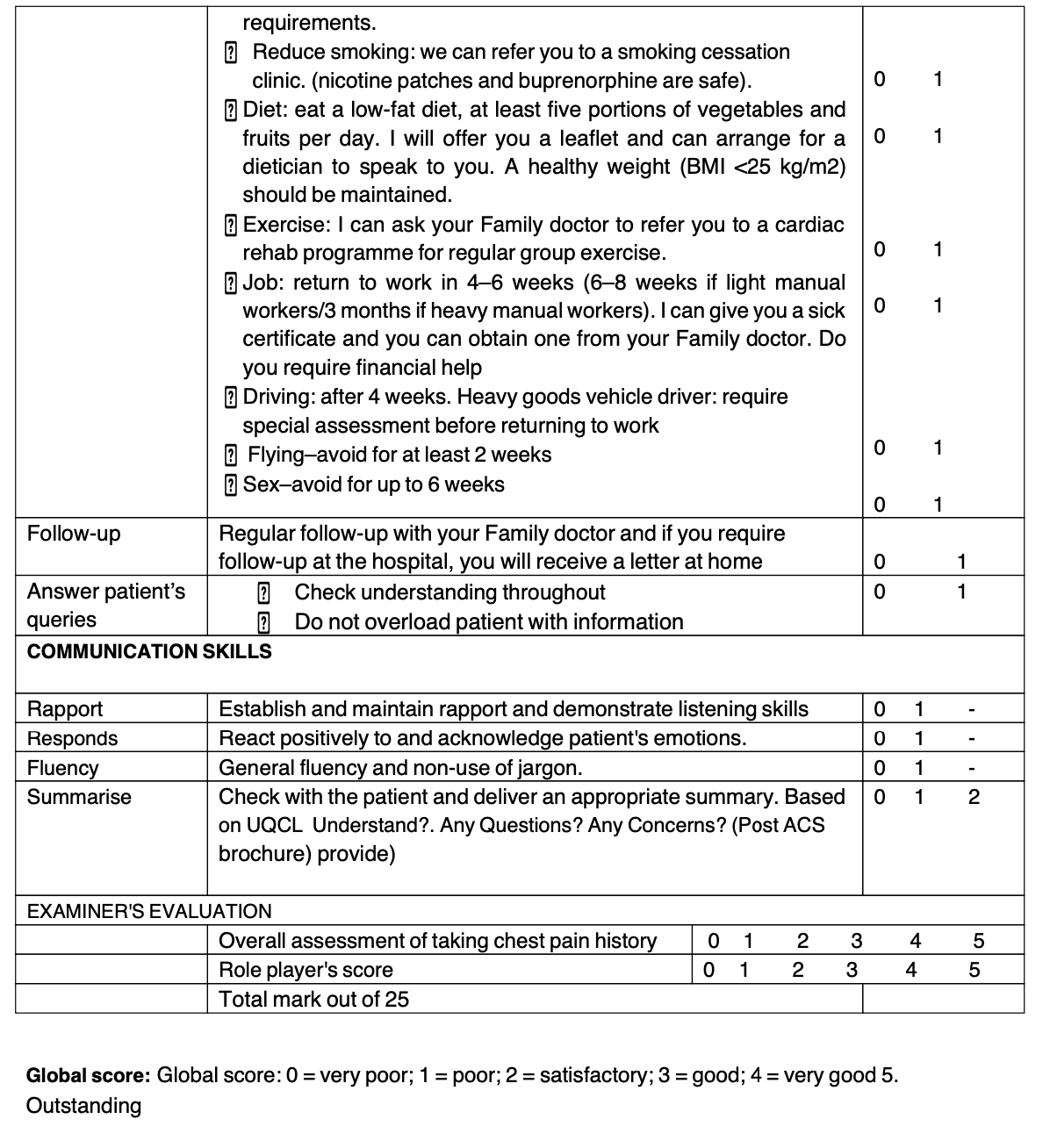 image source Med 1 Osce 2023 by
image source Med 1 Osce 2023 by
- Lina Serhan
- Alaa Alwerdani
- Leenah Turjoman
Station CCTD2
-
Introduce(cardiologist), purpose (consultation/advice)
-
take demographic data, past hx
-
ask if he knows his condition then explain if not with simple language
-
then give advice (depending on risk factor; diet smoking alcohol obesity exercise married sexual activity (Sildenafil) travel) to decrease further attacks
-
if he had attack again what he should do,
-
what are associated symptom,
-
importance of compliance with medication
khalaf, 57y, sudanese teacher, married (doesnt know about heart attack) cardiac ischemic issue perticipated by risk factors, genetics from occlusion of…
DM HTN CL - smokes 2 packs a day for 20 years he tried to stop but failed, doesnt drink, or use any recreational drug, no recent travel
-
we will give medications to reduce mortality,
-
controlling DM, HTN (BP), CL and use reliever GTN when symptoms appear, come to ER when…
-
avoid risk factors such as bad diet (processed food, low fiber), lack of exercise, smoking; try to go to cessation smoking center
-
Try avoid driving in upcoming 2w & 6wk small large veichle respectively,
-
6w with no sexual activity
-
Avoid traveling for 2 weeks
-
do you have any questions?
Station 2 A Communication and counselling stations. Dr Sami Scene: cardiology ward
Case scenario 1 A 52-year-old gentleman teacher with a history of angina. He has come in with severe chest pain, unrelieved by GTN. The ambulance crew gave them pain relief and did an ECG. The ECG looks like an acute STEMI.
Other cases?
Case 1
Find compromises without risking patients life when asked to cover shift - for example being in same hospital when complicated case appears or the student/resident doesnt know how to approach it etc.. be nice i guess
Case 2
Give blood to the child’s jehova witness and potentially go to jail after court
make sure to give signature first if denied just do it :)
Some of CCTD 1 & 2 not included here such as https://medatlax.com/Clinical/Level-9/Internal-medicine/IM-Case-Scenarios/CCTD1
https://medatlax.com/Clinical/Level-9/Internal-medicine/IM-Case-Scenarios/CCTD2