Internal Medicine
NSTEMI & UNSTABLE ANGINA
Investigations and Treatment
High risk patient who are likely to progress to MI require urgent coronary angiography in less than 72 Hours
Who are high risk patient ?
- Increased Troponin
- Dynamic ST or T wave changes
- Previous MI
- PCI within last 6 months
- Previous CABG
Medical Treatment Unstable Angina & NSTEMI
- O2 ⇒
- Morphine and anti emetic ⇒
- Aspirin ⇒
- Clopidrogrel (Plavix )- anti platelet agent OR : Dual AP therapy with Aspirin & Prasugrel or ticagrelor ⇒
- Enoxaprin- low molecular heparin ⇒
- Beta blocker ⇒
- (Bisoprolol) ⇒
- ACE-Inhibitors ⇒
- Nitrates ⇒
- Statins ⇒
FM
Unstable Angina / NSTEMI
Definition
“… ST-segment depression or prominent T-wave inversion and/or positive biomarkers of necrosis… in the absence of ST-segment elevation and in an appropriate clinical setting…”
Principal Presentations of Unstable Angina
| Class | Presentation |
|---|---|
| Rest angina* | Angina occurring at rest and prolonged, usually greater than 20 min |
| New-onset angina | New-onset angina of at least CCS class III severity |
| Increasing angina | Previously diagnosed angina that has become distinctly more frequent, longer in duration, or lower in threshold (i.e., increased by 1 or more CCS class to at least CCS class III severity) |
Patients with non–ST-elevated myocardial infarction usually present with angina at rest. Adapted with permission from Braunwald E. Unstable angina: a classification. Circulation 1989;80:410–4 (14).
CCS = Canadian Cardiovascular Society classification; UA = unstable angina.
Management Strategy for NSTEMI
Initial Therapy - MONA
- Morphine for pain
- Oxygen if hypoxic
- Nitro spray/drip for pain
- Aspirin
Management Strategy for NSTEMI/NST Chest Pain
- Establish risk level using the TIMI scoring system:
- Low risk: May be discharged after symptom control
- Moderate risk: Admit for further evaluation; add beta blockers, ACE inhibitors. Follow cardiac enzyme levels. If MI ruled out, Exercise or Adenosine stress test before discharge
- High Risk: Admit for cardiac catheterization
Treatment of Unstable Angina
- Antiplatelet therapy: Aspirin, clopidogrel, or both.
- Anticoagulants: A heparin (unfractionated or low molecular weight heparin).
- Antianginal therapy, usually nitroglycerin.
- Beta-blocker
- Angiotensin-converting enzyme (ACE) inhibitor
- Statin.
Thera
Unstable angina may present by one of the following:
- ~ Angina at rest
- ~ Crescendo angina (increased frequency and severity)
- ~ Angina of recent onset (within 4-6 weeks)
It may be due to:
• Non-occlusive coronary thrombus on top of atheroma. • Coronary artery spasm (Prinzmetal’s angina).
Unstable angina (UA) is considered to be present in patients with: ischemic symptoms suggestive of an ACS without elevation in biomarkers with or without ECG changes indicative of ischemia.
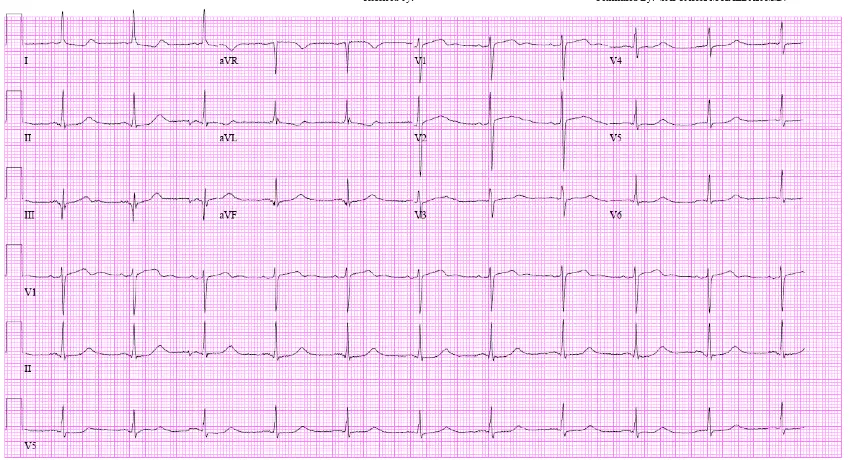
Diagnosis:
- ECG: shows changes in 30-50%.
- Cardiac enzymes: are not elevated distinguished from acute MI.
- Coronary angiography.