Meconium Aspiration Syndrome
One of the most common etiologies of respiratory failure in newborns. Occurs in term infants and SGA. Passage of meconium in utero is occurring because of relaxation of the anal sphincter.
Clinical Presentation
- Yellow-green staining of fingernails, umbilical cord, and skin may be observed.
- Meconium plugs the airways causing atelectasis. Meconium impairs surfactant production and function. It irritates the airways, causing chemical pneumonitis and possible secondary bacterial infection.
Symptoms include:
- Cyanosis
- Nasal flaring
- End-expiratory grunting
- Intercostal retractions
- Tachypnea
- Barrel chest in the presence of air trapping
- Auscultated rales and rhonchi
- Air leak
Severe MAS causes marked persistent pulmonary hypertension (PPHN) which develops and leads to right-to-left shunt at PFO & PDA with severe cyanosis. Almost 50% of meconium aspiration syndrome infants require mechanical ventilation.
Risk Factors
- Placental insufficiency
- Maternal hypertension
- Oligohydramnios
- Fetal distress / hypoxia (increases risk of MAS)
- Maternal drug abuse (e.g., cocaine)
- Maternal infection/chorioamnionitis
Complications
- Chemical pneumonitis (antibiotic = ampicillin and gentamicin)
- Respiratory distress syndrome (RDS)
- Pneumothorax
Management
Infants who are depressed at birth should be closely observed in a neutral thermal environment (incubator).
Monitor blood glucose, calcium, renal function, and electrolytes.
Clear secretions and meconium from mouth and nose using a bulb syringe or a large-bore suction catheter.
Continue routine neonatal resuscitation steps if the patient is active. Do not electively intubate!
If no response and hypoxia occurs:
- Oxygen therapy
- Surfactant therapy commonly used
- Mechanical ventilation

Medications to be Used
Antibiotics:
-
Differentiating between bacterial pneumonia and meconium aspiration by clinical course and chest x-ray may be difficult. So antibiotics (Ampicillin and gentamicin) are usually indicated. Blood cultures should be obtained to identify infections.
-
Endotracheal surfactant may improve oxygenation and reduce pulmonary complications and the need for ECMO.
Tricuspid regurge in echo, persistant pulm htn
Complications
-
Air leak (dangerous)
-
PPHN (dangerous)
-
Echocardiography should be performed to ascertain the degree of PPHN and to exclude congenital heart disease.
-
Pulmonary sequelae: Higher incidence of pneumonia, hyperinflation, consolidation, patchy infiltrates. If severe, air leak and pneumomediastinum may occur.
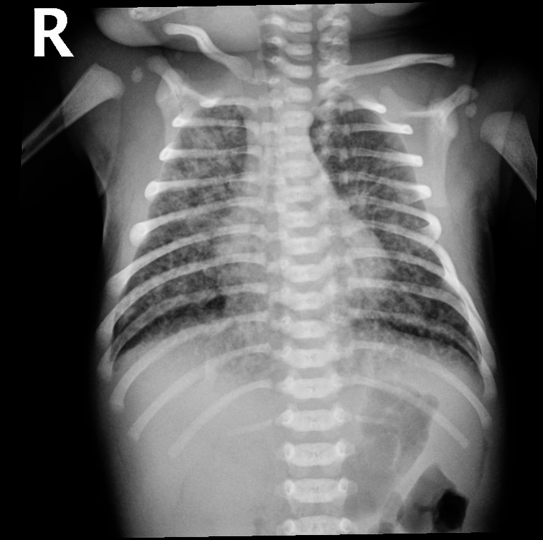
- Hyperinflation,
- Consolidation,
- Patchy infiltrates
- If severe, air leak and pneumomediastinum may occur
- Lines going from inside to outside