Surgery & Clinical Medicine
Carotid Body tumour(Syn. Chemodectoma, Potato Tumor)
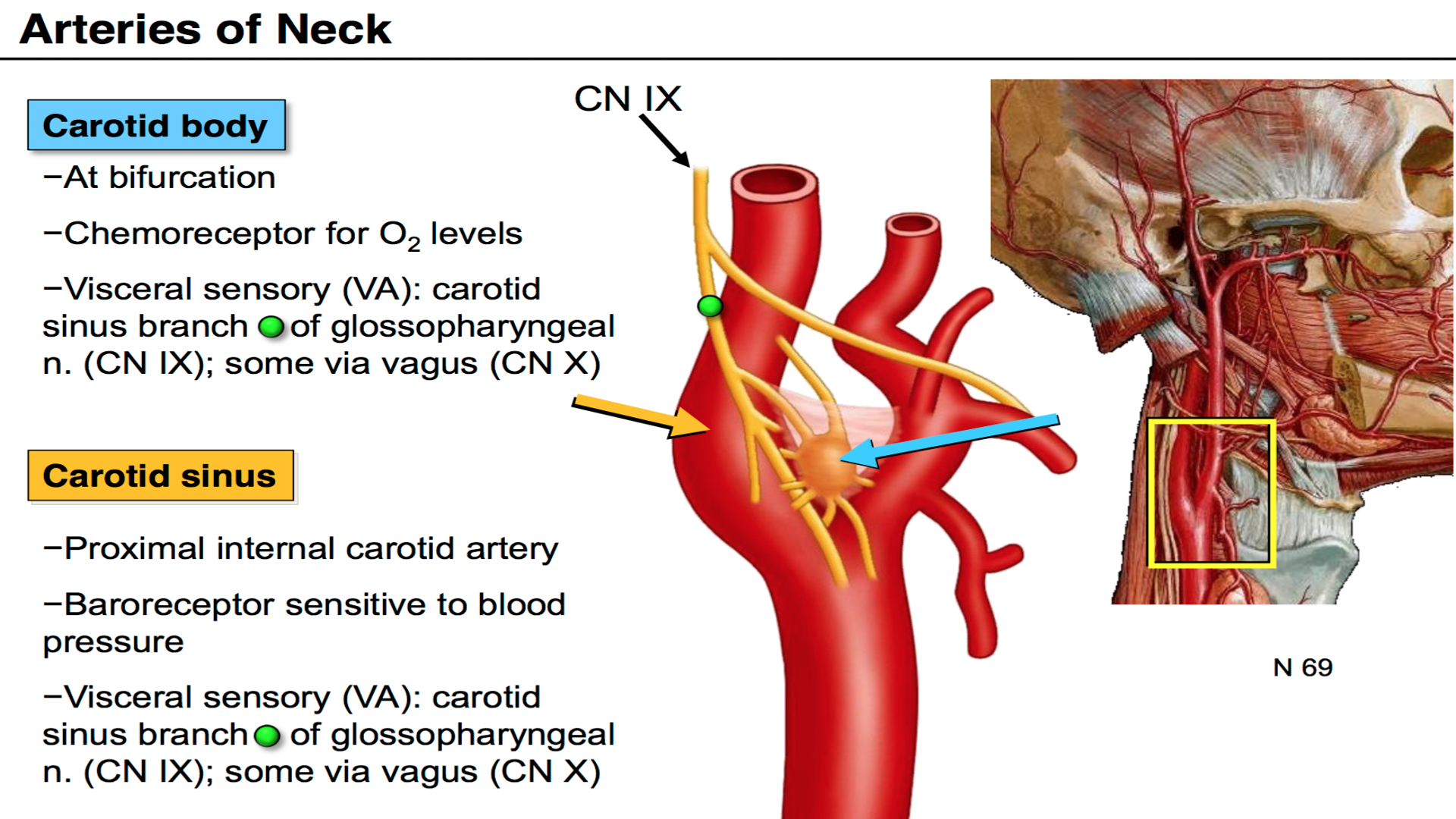
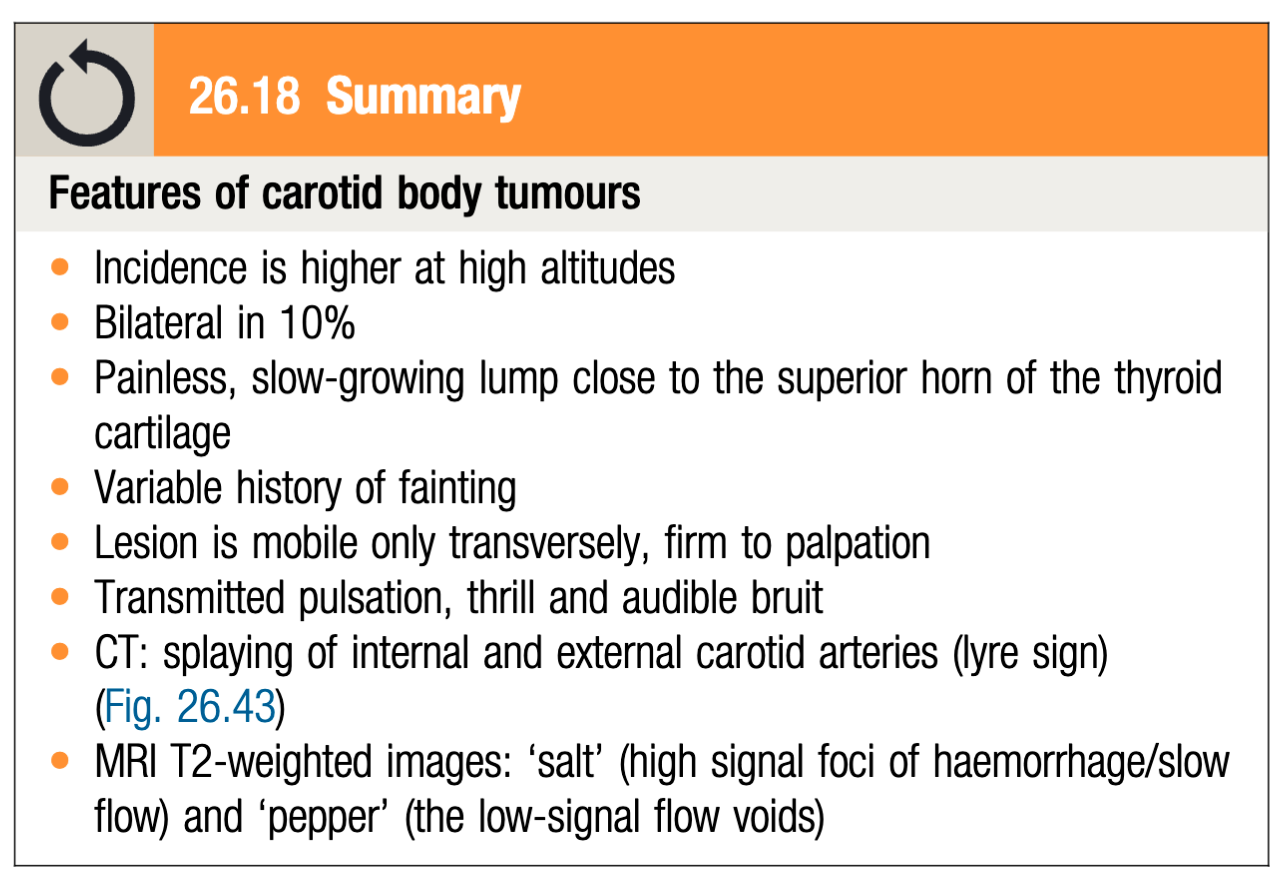
It is a slow growing tumor which arises in the carotid body at the carotid bifurcation, 2 – 10 cm, in size, well capsulated
A chemoreceptor organ which is stimulated by the rise in PCO2 or H+ ion concentration of arterial blood or a decline in its PO2.
Clinical Features:
-
Firm, homogeneous and compact tumor, like a potato.
-
Highest incidence is between the ages 40 and 60 years of life.
-
Slow growing painless swelling at the bifurcation of common carotid artery Z
-
Pressure on the carotid sinus from the tumor produces attacks of faintness.
Differential Diagnosis:
- Cervical lymph node enlargement.
- Sternomastoid tumor.
- Branchial cyst.
- Aneurysm of carotid artery.
Special investigation:
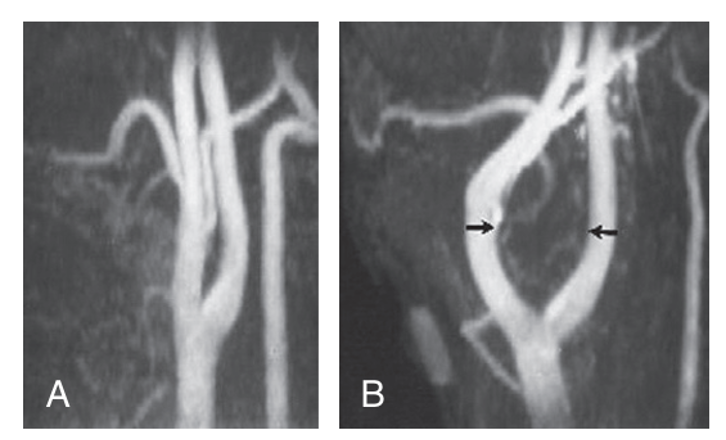
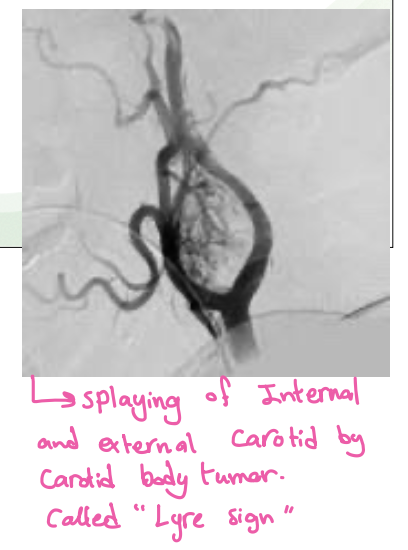
Arteriography-Shows the carotid bifurcation to be splayed open by the mass which is rich in vascularity

 What is Lyre sign in CT scan?
angiogram - most likely carotid body tumour
What is Lyre sign in CT scan?
angiogram - most likely carotid body tumour
Principles and practice of surgery source P. 527
Six genes have been associated with the development of paragan- glioma, including RET, VHL and NF1. Paragangliomas may also be hereditary, included as part of genetic syndromes such as von Hip- pel–Lindau, neurofibromatosis type I, MEN 2A and MEN 2B. Spo- radic cases may be caused by germline mutations. The three most common paragangliomas in the head and neck region are carotid body tumour, glomus jugulare and glomus intravagale. The carotid body is located in the adventitia of the posteromedial aspect of the carotid bifurcation. Its chemoreceptors regulate ventilation in response to changes in arterial blood gases and pH. 26.18
Angiography is useful to define (and possibly embolise) the feeder vessels. Biopsy is hazardous because of the risk of bleeding and formation of a pseudoaneurysm. About 5–10% of these tumours are malignant. A diagnosis of malignancy is based on lymph node or distant metastases as pathology. Histopathological criteria are unreliable to make a diagnosis of malignant carotid body tumour. Treatment is surgical excision. Operative bleeding and duration of surgery are reduced by preoperative embolisation. Occasion- ally, vascular repair of the carotid artery is required. Preoperative balloon occlusion studies can be used to assess the cerebral blood flow. The tumour may be excised by dissecting in the sub- adventitial plane. The superior laryngeal nerve, vagus nerve and hypoglossal nerve are at risk during the procedure. In bilateral lesions, operate on the smaller first and counsel the patient that there may be fluctuation in blood pressure following the second side excision due to complete loss of carotid sinus function. It is estimated that malignant paragangliomas have less than a 50% 10-year survival rate; surgery is the treatment of choice as chemotherapy and radiation do not appear to be of significant benefit.