IM
Dr.waqar
Definition of autoimmune disease
Autoimmune diseases are conditions in which antibodies are formed against the person’s own body tissues In some diseases, ab. are formed against one organ only ( DM type1, Grave’s disease) while in others, ab. are formed against many tissues
DEFINITION OF SLE
SLE is an autoimmune disease in which antibodies are formed against many tissues of the body ( multisystem disease). These antibodies cause damage and inflammation in the tissues.
EPIDEMIOLOGY
- Geographics : Occurs worldwide
- Gender : F:M ratio is 9:1 ( usually young women, aged 20 to 40).
- Race : More in black Americans
ETIOLOGY
Like most autoimmune diseases, cause is unknown but some associations are observed:
- If one twin is affected, more chances in the other ( ? Genetic role)
- More chances in 1st degree relatives
- More chances in premenopausal women ( ? may be hormonal cause)
- Some drugs can cause SLE like picture: INH; TB Hydralazine; antihypertensive; pregnancy Penicillamine
S/S
S/S of SLE are “very” varied & may be mild to severe. SLE can affect any organ BUT REMEMBER 3 MOST COMMON FEATURES Fatigue & malaise Muscle & joint pain Fever
- 1) Gen. features: Fatigue, fever, wt loss
- 2) Joint & Muscles:
*Pain in small joints of hands ( like R.A.) * Other joints may also be affected * Usually no joint swelling * Myalgias - 3) Scalp: hair fall, discoid alopecia
- 4) Brain: cerebritis, psychosis, depression
- 5) Eyes: Retinal infarcts, scleritis
- 6) Mouth: Ulcers
- 7) Skin rash: Skin is affected in 85% patients Butterfly rash Discoid rash Butterfly rash is characteristic of SLE SLE rash gets worse in sunlight (photosensitive)
Sometimes discoid skin lesions are seen

SKIN RASH IN SLE ⇒ Butterfly rash on the face a) involves the cheeks, b) crosses over the nasal bridge c) no involvement of the nasolabial fold d) May be slight pain or HAKKA
-
8) Lungs:
- pleuritis, pleural effusions
- Interstitial lung disease
-
9) Heart: * Pericarditis * Myocarditis
- Non bacterial endocarditis of the mitral valve ( Libman-Sacks endocarditis)
- Increased risk of coronary artery disease (angina, MI)
-
10) Raynaud’s phenomenon:
-
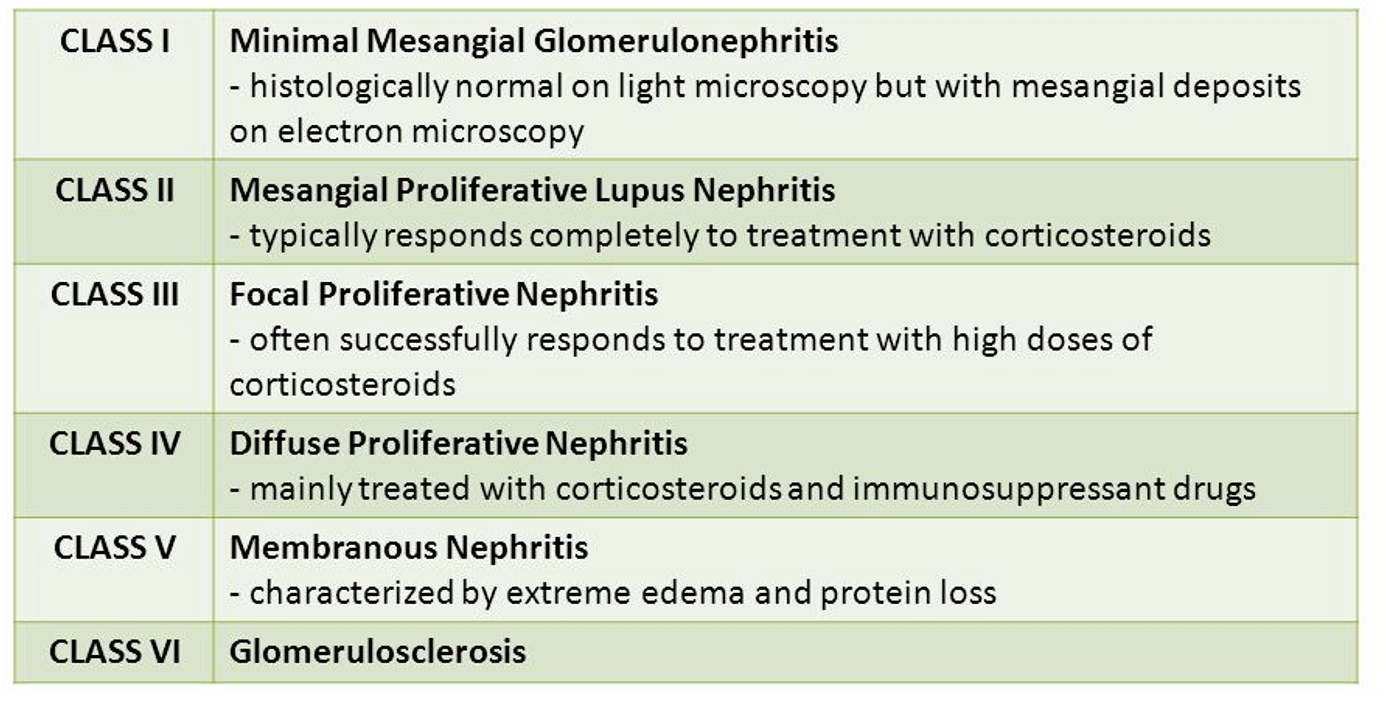
11) Kidneys( Lupus nephritis) : SLE causes various types of glomerulonephritis which present as either nephrotic syndrome or nephritic syndrome. W.H.O. has classified lupus nephritis into 6 classes based on histology of the renal lesion (class 1 to 6).
-
Class 4: Most common renal lesion in SLE & causes nephritic syndrome called diffuse proliferative (GN) or Membrano-proliferative GN (MPGN)
-
Class 5: Also called Membranous nephropathy (MN). Causes nephrotic syndrome. SLE NEPHRITIS HAS HIGH MORBIDITY & MORTALITY
-
WHO class of Lupus Nephritis
1) Routinely check urine in SLE patients. If any
blood or protein, investigate further ( biopsy)
2) Treatment of lupus nephritis depends on the
class of lesion which is present, so biopsy is
important.
- 12) GIT: Vasculitis of the intestinal vessels causing bowel infarction
- 13) Blood vessels: Vasculitis anywhere
- 14) BLOOD:
- Anemia
- Low WBC
- Low platelets (antibodies are formed against RBC, WBC & platelets)
INVESTIGATIONS
- CBC : *Anemia * Low WBC * low plts.
- Urea/creatinine :
- Raised in advanced renal disease ( lupus
nephritis)
- Raised in advanced renal disease ( lupus
- **3) Urine : ** * may show proteins & blood
- 4) ESR: Raised in acute flare
- 5) C3, C4 (complements) : reduced in acute flare & lupus nephritis
- 6) Autoantibodies : Important ones are : a) ANA (antinuclear ab.) : Present in almost all pts. Not specific for SLE but done as the first screening step. Titers should be at least 1:80 ( if ANA negative, SLE is ruled out)
Done only if ANA is positive
b) Anti double stranded DNA ( anti ds DNA) ( * v. specific for SLE - Present in 70% pts., only specially during acute flare)
c) Anti Sm ab. : most specific
d) Anti Ro, anti La
- **7) Renal Biopsy : **
- Done if nephritis is suspected ( abn. urine)
- Shows the class of renal disease, which helps us decide about drugs
WHEN TO SUSPECT SLE
- Consider SLE in a female with multisystem symptoms
- Confirm with blood tests
- Rheumatology consultation for all patients
Points about drug induced Lupus
- No CNS, renal or major organ involvement
- ANA & anti-histone ab. positive
- Can occur even years after starting the drug
- Resolves after stopping the drug
- Common symptoms -⇒ fever, arthralgias, myalgias, mild pleuritis
DIAGNOSTIC CRITERIA
American College of Rheumatology has 11 criteria, at least 4 of which should be present to diagnose SLE. BUT These criteria were meant to enroll patients in clinical trials, not to diagnose individual patients.
TREATMENT
THERE IS NO CURE FOR SLE Drugs used:
- Hydroxychloroquin; rheumatology, protective, malaria
- NSAIDs; as needed
- Glucocorticoids;
- Immunosuppressive drugs; ( Cyclophosphamide, Mycophenolate mofetil, Methotrexate, Azathioprine).Used for long term control of the disease.
- Belimumab (a monoclonal antibody)
Hydroxychloroquin is given long term to almost all symptomatic patients. For mild symptoms, this is enough.
In case of moderate to severe symptoms or major organ involvement, steroids, immuno-suppressives & /or monoclonal antibodies are added
-
**Fatigue, arthralgias, fever, pleuritis **
- Hydroxychloro;Can cause retinal toxicity, so regular eye checks
- NSAIDs
-
Skin rash:
- Topical steroids
- Sunscreens
- Hydroxychloroquin tabs.
- Sometimes, oral steroids may be needed
-
Avoid long sun exposure ( SLE gets worse in sun)
-
Periods of rest during acute flares
Treatment of Nephritis
- Steroids
- Immunosuppressives (eg Mycophenolate, azathioprine, methotrexate, cyclophosphamide)
- Sometimes, monoclonal antibodies are also added.
- Treatment may be long term
The following features in SLE also need aggressive treatment with steroids/ immunosuppressants: a) Cerebritis b) Anemia, low WBC, low platelets
COURSE OF SLE
Most patients have relapsing-remitting course
Features of an acute flare:
- Worsening of signs/symptoms
- Rise in ESR
- Fall in blood complement levels (C3, C4)
- Further rise in anti-ds-DNA ab. levels
PROGNOSIS
- Mortality has fallen dramatically in the last 50 yrs due to advanced Rx.
- 10 yr survival rate is 90%
- Causes of death :
- Coronary artery disease: No. 1 cause of death
- Renal disease
- CNS disease
- Autoimmune hemolytic anemia
PREGNANCY & SLE
- Fertility is normal but increased chances of miscarriage and fetal death
- SLE is not a contraindication to pregnancy but tell the patient about the risks
- Exacerbations can occur during pregnancy & even after delivery
- Corticosteroids, azathioprine & hydroxychloroquine are safe in preg.
There is no increased risk of neonatal lupus related to breastfeeding. However, some medications enter breast milk: Nonsteroidal antiinflammatory drugs (NSAIDs) can be used, but high-dose aspirin should be avoided. Prednisone can be taken.
RAPID FIRE QUESTIONS
-
Most common symptoms of SLE?
- Fatigue
- Joint pain
- Skin rashes
- Fever
-
Most common rash?
- Malar rash (butterfly rash)
-
Features of the most common rash?
- Erythematous
- Involves the cheeks and bridge of the nose
- Spares the nasolabial folds
-
Treatment of the rash?
- Topical corticosteroids
- Sun protection
-
Features in the heart?
- Pericarditis
- Libman-Sacks endocarditis
-
Which antibiotic to use in SLE endocarditis?
- Typically, antibiotics are not used; treatment focuses on managing SLE with immunosuppressants.
-
Features in the brain & lungs?
- Brain: Seizures, psychosis
- Lungs: Pleuritis, interstitial lung disease
-
What happens during pregnancy?
- Increased risk of complications such as preeclampsia, preterm birth, and fetal loss
-
Commonest cause of death in SLE?
- Cardiovascular disease
- Infections
-
Treatment of renal SLE?
- Immunosuppressants (e.g., corticosteroids, cyclophosphamide)
- ACE inhibitors or ARBs for proteinuria
-
Which drug to be given to all SLE patients?
- Hydroxychloroquine
-
Which drugs can cause SLE?
- Procainamide
- Hydralazine
- Isoniazid
-
Any 2 features of acute flare?
- Fever
- Worsening of rash or joint pain
CASE 1
A 35 year old lady presents with pain and swelling in the right lower leg since 2 days. Past history of recurrent abortions Had a stroke 2 years ago Also had popliteal artery thrombosis few years ago
APA Syndrome
Some patients with SLE have a condition called Antiphospholipid antibody syndrome ( APA syndrome, APLS)
It is an autoimmune condition where there are some abnormal antibodies in the blood, which cause thrombosis in blood vessels. Thrombosis can occur anywhere in the body (arteries or veins)
Dermatology
The “butterfly” rash
Butterfly rash: think rosacea or seborrheic dermatitis first
- Many facial rashes are described as “malar” or “butterfly” rashes
- Most “butterfly” rashes are seborrheic dermatitis or rosacea, not lupus, which is classically described as “malar” or “butterfly”

The “butterfly rash” of lupus




Key elements of facial lupus rash
-
Four SLE criteria are dermatologic:
- Photosensitivity
- Discoid lesions
- Oral ulcerations
- Malar rash
-
Photodistributed
-
Often scaly, scarring
-
Spares nasal creases (unlike seborrheic dermatitis)
-
May mimic rosacea
-
Refer these patients
