Physiological Changes in Pregnancy
By Dr. Mona Ahmed
Diagnosis of Pregnancy – Systemic Changes in the Pregnant Woman
Reproductive System Changes
- Anatomical and physiological changes to accommodate the changes and development of the fetus.
- These changes are presented as follows:
1. Uterus
- Uterine muscle fiber hypertrophy and hyperplasia
- With pregnancy progression:
- The uterus leaves the pelvic cavity and experiences increased size (five times more than normal).
- Blood supply increase to the uterus.
- Its weight increases from 70 gms to 1000gms.
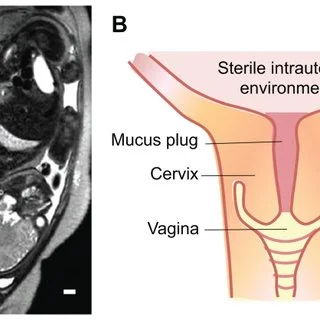
2. Cervix
- Enlargement of mucous glands secrete mucus which acts as:
- A seal for the uterus:
- Protects the cervix from ascending infection (barrier between it and the vagina).
- Later in pregnancy, before delivery, there is a softening of the cervix in response to the increasing uterine contractions. Labor Sign
- A seal for the uterus:
3. Vagina
- Increase in the blood supply to the vagina.
4. Vulva
- Increase vascularity leading to increased varicosity and varicose vein formation.
Breast Changes
- Increase skin thickening over nipple.
- Ducts - Proliferation of glandular epithelium of alveoli.
- Increase Vascularity & Dilated veins.
- Colostrum formation.
- Striae of skin.
- Nipples:
- Thick skin of nipple.
- Increase Pigmentation. secondary areola.
Cardiovascular System
Cardiac output increases: COP ↑
- Throughout early pregnancy.
- Peaks in the third trimester, usually to 30-50% above baseline.
- The Cause mediates the rise in cardiac output to 90.
- Overall blood volume increases by 40–50%.
- The heart rate increases (not above 100 beats/minute).
Total systemic vascular resistance decreases by 20% due to the vasodilatory effect of progesterone to increase blood flow. An increase in resistance Pregnancy-induced HTN.
Overall Systolic and diastolic blood pressure:
- Drops (10–15 mm Hg) in the 1st trimester.
- Then returns to the baseline in the 2nd half of pregnancy.
All of these cardiovascular adaptations can lead to common complaints, such as:
- Palpitations.
- Decreased exercise tolerance.
- Dizziness.
High BP in 1st trimester:
- HTN.
- Pregnancy-induced HTN.
Respiratory Changes
-
There is increasing edema in the upper airway tract, necessitating intubation with a smaller endotracheal tube
-
Elevated diaphragm by about 4cm due to uterine enlargement, especially in late gravida.
-
Ligaments connecting ribs to sternum become lax due to the effects of relaxin and progesterone, increasing the subcostal angle.
-
Increase in chest circumference (5-7cm), leading to lower chest compliance.
Lung Volume Changes
- Functional residual capacity decreases.
- Expiratory reserve volume decreases.
- Residual volume decreased.
- The total lung capacity decreases.
- Increase in the respiratory capacity.
- Respiratory rate increases.
- Increase in the tidal volume.
- Increase in oxygen consumption & the metabolic rate, more importantly responsible for the symptoms.
Gastrointestinal Changes
- Progesterone causes smooth muscle relaxation, which:
- Slows down GI motility.
- Decreases lower esophageal sphincter (LES) tone.
The resulting increase in intragastric pressure combined with lower LES tone leads to gastroesophageal reflux.
- Nausea and vomiting of pregnancy “morning sickness” is one of the most common GI symptoms of pregnancy.
- Relaxation of smooth muscle of the stomach.
- Constipation. Eating in small amounts is recommended.
- Hemorrhoids can occur during pregnancy. Progesterone VD.
Renal Changes
Increase in the size of the kidneys and ureter due to the increased blood volume and vasculature.
Later in pregnancy, women might develop physiological hydronephrosis and hydroureteronephrosis due to the reflux in the ureter caused by uterine pressure.
There is an increase in glomerular filtration rate (GFR) with an increase in:
- Creatinine clearance.
- Protein.
- Albumin excretion.
- Urinary glucose excretion.
Sodium Retention and Related Changes
- Increase in sodium retention: oxytocin mimic, ADH.
- Oedema.
- Water retention (a common sign in pregnant women).
In the third trimester, when the fetus engages in the pelvis, there is an increased frequency of urination and incontinence.
Increase Clearance of:
- Urea.
- Uric acid.
- Amino acids.
- Folic acid.
- Renin.
Glycosuria (due to increased glucose clearance) is normal in pregnant ladies if other tests are normal.
Nutrition
During pregnancy, protein and carbohydrate metabolism are affected.
One kilogram of extra protein is deposited, with half going to the fetus and placenta and another half going to:
- Uterine contractile proteins.
- Breast glandular tissue.
- Plasma protein.
- & haemoglobin.
The weight should increase.
Changes in Metabolism and Nutrient Requirements
An increased requirement for nutrients is driven by:
- Fetal growth.
- & fat deposition.
Changes are caused by diabetogenic hormones:
- Steroid hormones.
- Lactogen the cause of diabetes induced by Pregnancy.
- Cortisol.
Pregnant women require an increase in calories.
There is weight gain.
Weight Gain in Pregnancy
Increased weight is due to (Fetal causes):
- Fetus.
- Placenta.
- Amniotic Fluid.
Maternal causes:
- Uterus.
- Breasts.
- Blood volume.
- Fat and Protein storage.
- Water storage.
Weight gain varies between 7-17kg in normal cases.
Effects of Progesterone
- Reduces smooth muscle tone.
- Stomach motility diminishes…(nausea).
- Colonic activity reduced…(constipation).
- Reduced uterine tone…diminished uterine activity to prevent labor.
- Reduced bladder and ureteric tone…stasis of urine UTI.
- Reduces vascular tone…diastolic pressure reduced.
Pituitary Gland: Hypertrophy
An increase in:
- ACTH.
- Thyrotropin.
- Melanocyte hormone acanthosis nigricans hyperpigmentation.
- Prolactin.
FSH, LH Decrease to prevent menses.
Thyroid Glands: Physiologic Goiter
- TSH, FT4 T4, T3 Normal.
- Slight increase in thyroid gland size due to HCG mimicking TSH.
Immune System and Other Changes
- Immune suppression.
Musculoskeletal:
- Smooth Muscles Relaxation.
Skin:
- Increase pigmentation.
- Striae Gravidarum.
- Linea nigra.
Hands:
- Palmar erythema.
- Spider naevi.
Face:
- Chloasma (Melanocyte stimulating hormone).
Emotional Change:
- Depression due to hypercirculation.
Early Pregnancy Symptoms
- Missed Period.
- Faintness.
- Food Aversion.
- Tender Breasts.
- Nausea.
- Constipation.
- Frequent Urination.
- Slight Bleeding.
- Mood Swings.
- Fatigue.
- Raised Temperature.
- Headache.
Summary of Physiological Changes in Pregnancy
| Section | Main Points / Key Changes |
|---|---|
| Diagnosis of Pregnancy – Systemic Changes | Overview of systemic adaptations; includes image Physiological changes in Pregnancy-ps1-1.webp |
| Reproductive System | |
| • Uterus | Hypertrophy + hyperplasia; size ↑ ≈ 5 × ; weight 70 g → 1000 g; ↑ blood supply |
| • Cervix | Enlarged mucus glands → seal; softening before labor (labor sign) |
| • Vagina | ↑ blood supply |
| • Vulva | ↑ vascularity → varicosities, varicose veins |
| Breast | Skin thickening over nipple; glandular epithelium proliferation; ↑ vascularity & dilated veins; colostrum formation; striae; ↑ pigmentation of areola |
| Cardiovascular System | Cardiac output ↑ 30‑50 % (peak 3rd trimester); blood volume ↑ 40‑50 %; HR ↑ (≤ 100 bpm); SVR ↓ ≈ 20 % (progesterone‑mediated); SBP/DBP ↓ 10‑15 mm Hg in 1st trimester then returns; common symptoms: palpitations, ↓ exercise tolerance, dizziness |
| Respiratory Changes | Upper‑airway edema → smaller ET tube; diaphragm ↑ ≈ 4 cm; ribs‑sternum laxity ↑ subcostal angle; chest circumference ↑ 5‑7 cm → lower compliance |
| Lung Volume Changes | ↓ FRC, ↓ ERV, ↓ RV, ↓ TLC; ↑ respiratory rate, ↑ tidal volume, ↑ respiratory capacity, ↑ O₂ consumption & metabolic rate |
| Gastro – GI Changes | Progesterone‑induced smooth‑muscle relaxation → ↓ GI motility, ↓ LES tone → reflux; “morning sickness”, constipation, hemorrhoids |
| R enal Changes | ↑ kidney & ureter size; possible physiologic hydronephrosis; GFR ↑ → ↑ creatinine clearance, protein, albumin, glucose excretion |
| Sodium Retention & Related | ↑ sodium & water retention (oxytocin/ADH); edema; ↑ urination & incontinence in 3rd trimester |
| Increased Clearance of | Urea, uric acid, amino acids, folic acid, renin; glycosuria may be normal |
| Nutrition | ↑ protein & carbohydrate metabolism; 1 kg extra protein split between fetus/placenta and maternal tissues (uterus, breast, plasma, Hb) |
| Metabolism & Nutrient Requirements | ↑ caloric need; driven by fetal growth & fat deposition; diabetogenic hormones (steroids, lactogen, cortisol) raise glucose demand |
| Weight Gain | Total 7‑17 kg (↑ fetal, placental, amniotic fluid + maternal uterus, breasts, blood, fat/protein, water) |
| Progesterone Effects | ↓ smooth‑muscle tone → ↓ stomach motility (nausea), ↓ colonic activity (constipation), ↓ uterine tone (prevent premature labor), ↓ bladder/ureter tone (UTI risk), ↓ vascular tone (↓ diastolic BP) |
| Pituitary Hypertrophy | ↑ ACTH, TSH, MSH (→ hyperpigmentation), prolactin; ↓ FSH/LH (prevent menses) |
| Thyroid – Physiologic Goiter | TSH, FT4, T3 normal; slight gland enlargement due to HCG mimicry |
| Immune & Other Changes | Immune suppression; musculoskeletal smooth‑muscle relaxation; skin ↑ pigmentation, striae gravidarum, linea nigra; hands → palmar erythema, spider naevi; face → chloasma; mood → depression (hypercirculation) |
| Early Pregnancy Symptoms | Missed period, faintness, food aversion, tender breasts, nausea, constipation, frequent urination, slight bleeding, mood swings, fatigue, low‑grade fever, headache |