Examination of the Shoulder
Prof. Mamoun Kremli
Orthopedic Examination
Which system to use?
- Look
- Feel
- Move
- Special tests
Look
General on patient
General local – shoulder, arm, upper limb
- Position
- Major deformity- swelling
- Extra – cast, splint, traction, dressing …
Anatomic local
- Skin : swelling, scars, colour, hair, dryness …
- Subcut. : LN, veins, nerves, tendons …
- Muscles : bulk, wasting, twitches …
- Bones : landmarks, swelling, angulation and deformity.
- Joints : position, swelling, redness..
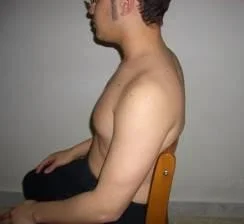
Look
General on patient :
- Lying comfortably in bed, not in pain.
- Lying in bed in pain keeping the R upper limb on his chest.
- Standing with the R shoulder adducted and internally rotated and elbow extended.
- Sitting uncomfortably in a chair with R forearm in an arm sling.

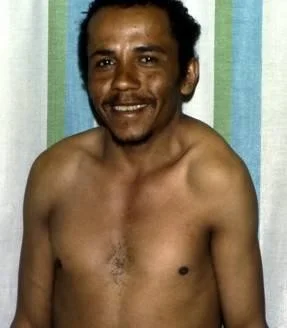
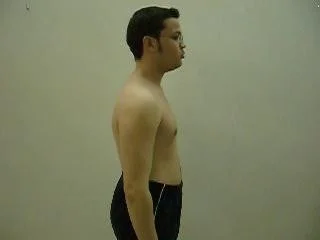
Inspection from multiple angles
- Anterior
- Posterior
- Lateral
- Above
- Axilla





Look
General local
Shoulder - Arm - Upper Limb
-
Position
- Abduction
- Adduction
- Flexion
- Rotation
-
Major deformity- swelling
- Contour
- Masses
- Asymmetry
Shoulder - Arm -Upper Limb
- Extra
- Cast
- Splint
- Traction
- Dressing …

Anatomic local
- Skin : swelling, scars, colour, hair, dryness …
- Subcut. : LN, veins, nerves, tendons …
- Muscles : bulk, wasting, twitches …
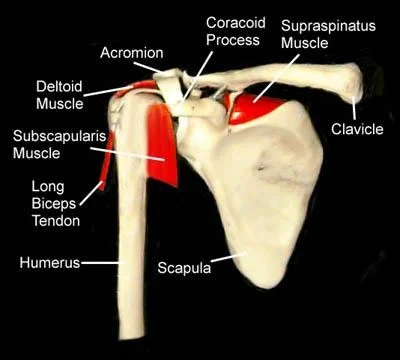
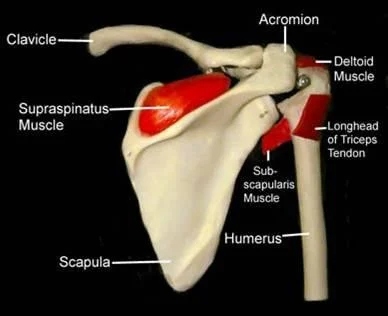
- Bones : landmarks, swelling, angulation and deformity
- (sterno-clavicular, acromio-clavicular, greater tuberosity, scapula)
- Joints : position
- (Don’t forget Posterior / Lateral / Superior !)
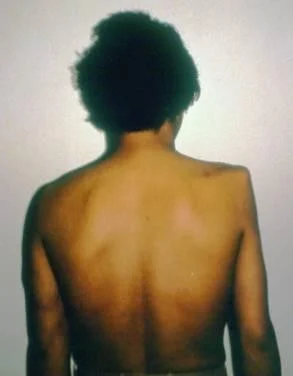
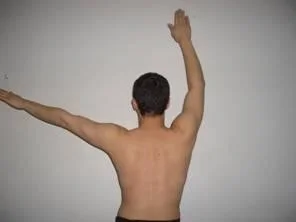
Anatomic local
- Muscles : bulk, wasting, twitches
- With the patient sitting, look for atrophy in three sites:
- The supraspinatus fossa
- The infraspinatus fossa
- The deltoid
- This demonstrates weakness due either to a rotator cuff tear, or a neurological deficit.
Anatomic local
Bones / Joints:
- landmarks, swelling,
- angulation and deformity.
- Sterno-clavicular joint.
- Clavicle.
- Acromio-clavicular joint.
- Greater tuberosity.
- Scapula and scapular spine

Important Considerations:
- Amount of exposure
- Duration of exposure
- Persons present during exposure
- Place of exposure
- Attitude and behavior during exposure
Feel
-
Tenderness:
- Generalized / specific
-
Temperature:
- compare distal/proximal, compare Rt/Lt
-
Anatomic:
- Skin : dryness, hyper/hypothesis, scars
- Subcut. : LN, nerves, vessels, tendons, nodules
- Muscle : tone, bulk, twitches, gaps, tenderness
- Bone : tenderness, mass, crepitus, landmarks: ( Sternoclavicular, Acromioclavicular, Coracoid Process, Greater Tuberosity, scapular spine, and scapula ).
- Joint : swelling, effusion, crepitation, synovial thickening, joint line tenderness.
Specific areas to examine
-
Acromio-clavicular Jt.

-
Bicipital groove

Move
- Shoulder joint motion is associated with Scapulo-thoracic motion
- Practically we deal with BOTH as one joint
- Active / Passive
- Start with active range of motion
- Supplement with passive if active not full
Movement Directions (normal range)
- Abduction (150°)
- Forward flexion (180°)
- Extension (45°)
- External Rotation (90°), elbow at 90°
- With arm comfortably at side
- With arm at 90o abduction
- Internal rotation (90°)
Move: Flexion / Extension



Move: Abduction / Adduction



- Look at :
- Range of motion
- Smoothness of motion
- Painful motion

Move: Abduction / Adduction
-
Shoulder abduction involves the gleno-humeral joint and the scapulo-thoracic articulation
-
The first 20° - 30° of abduction should not require scapulo-thoracic motion
-
active abduction:
- Initiation, range, rhythm
-
Note the arc of painful movement - Painful Arc
- Initiation of abduction: Supraspinatus
- Middle abduction (30°–90°): Rotator cuff
- Extreme abduction (>90°): Acromio-clavicular
- active abduction:
- Note the arc of painful m
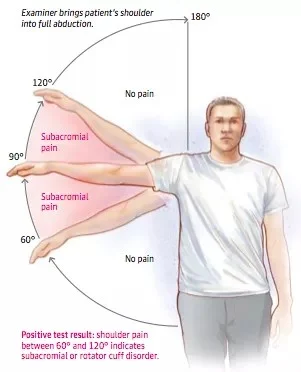
Positive test result: shoulder pain between 60° and 120° indicates subacromial or rotator cuff disorder.
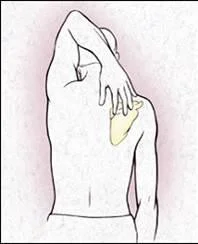
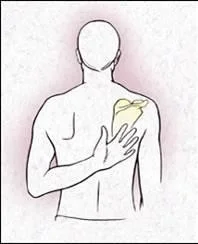
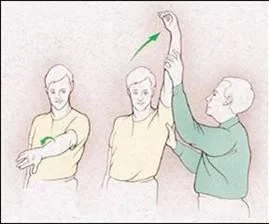
Move: Internal / External Rotation
- Apley’s Scratch Test
- Abduction and External & Internal Rotation


-
1- limited, 2,3 normal


-
• In neutral position
-
• Keep elbow at patient’s side

-
In neutral position
-
Keep elbow at patient’s side

- In abduction



• In Abduction

Special Tests
- Apprehension test
- Impingement tests
- Muscle power tests
- Axillary nerve assessment
Apprehension test
- Technique
- Patient’s Start Position:
- Elbow flexed 90 degree
- Shoulder abducted 90 degree
- Apprehension Maneuver:
- Examiner holds patient’s wrist
- Apply forward pressure from beh
- Externally rotate shoulder
- Positive if causes apprehension
- Patient’s Start Position:



Neer’s Impingement Test
- Tests for impingement of the rotator cuff tendons under the coracoacromion
- Internally rotate the arm with
- the thumb facing downward
- Abduct and forward flex
- the arm
- If impingement is present,
- the patient will experience
- pain as the arm is abducted


Hawkins’ Impingement Test
-
Tests for subacromial impingement or rotator cuff tendinitis.
-
The arm is forward elevated to 90 degrees, then forcibly internally rotated.
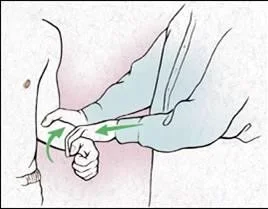
Yergason Test (Biceps tendon)
- Test for biceps tendon instability or tendinitis
- The patient’s elbow is flexed to 90
- The examiner resists the patient’s attempt to supinate the arm and flex the elbow

Special Tests
- Muscle power tests:
- Abductors / Adductors
- Internal / External Rotators
- Serratus Anterior (winging)
- Biceps Brachii
Muscle power
External / Internal Rotators Strength Test



Supraspinatus Test
- Assess power and for look for pain on resisted action


Serratus Anterior - Scapular Winging
- Nerve to Serratus Anterior –

- The Long Thoracic Nerve

Special Tests: Biceps Tendon
- Look for tenderness / pain on resisted action

- Ruptured long head.

Axillary nerve assessment
- Motor : active abduction (Deltoid)
- Sensory : upper lateral aspect of arm
Summary
- Shoulder examination follows the usual
- Look, Feel, Move, Special tests
- Active motion is more important
- Gleno-humeral and scapulo-thoracic together
- Special tests:
- Apprehension test
- Impingement tests
- Muscle power tests
- Axillary nerve assessment