SURGERY
Colonic polyps
- Slow-growing overgrowths of the colonic mucosa.
There are two main categories of polyps:
-
Non-neoplastic:
- Hyperplastic polyps,
- Inflammatory polyps
- Hamartomatous polyps.
-
Neoplastic
- Adenomatous
- Adenomatous type is important:
- Most common type of polyps
- Associated with malignant risk
Malignant risk is associated with
- Degree of dysplasia
- Type of polyp:
- Tubular Adenoma: 5% risk of cancer (Commonest)
- Tubulovillous adenoma: 20% risk of cancer
- Villous adenoma: 40% risk of cancer
Size of polyp:
- < 1 cm =<1% risk of cancer
- 1-2 cm=10% risk of cancer
-
2 cm=50% risk of cancer
| Histologic type | Tubular adenomas | Villous adenomas | Tubulovillous adenomas |
|---|---|---|---|
| Characteristics | characterized by a complex network of branching adenomatous glands | contain fronds or folds of mucosa that have overgrown their underlying stroma and project toward the colonic lumen | both histologic types coexist |
| % of total adenomatous polyps | 65%-85% (most common) | 5% 10% (least common) | 10%-25% |
| Malignant potential | 5% (have less atypia) | 40% (have severe atypia) | 22% |
| Location | Found anywhere in colon | Found mostly in rectum | Mostly in rectum |
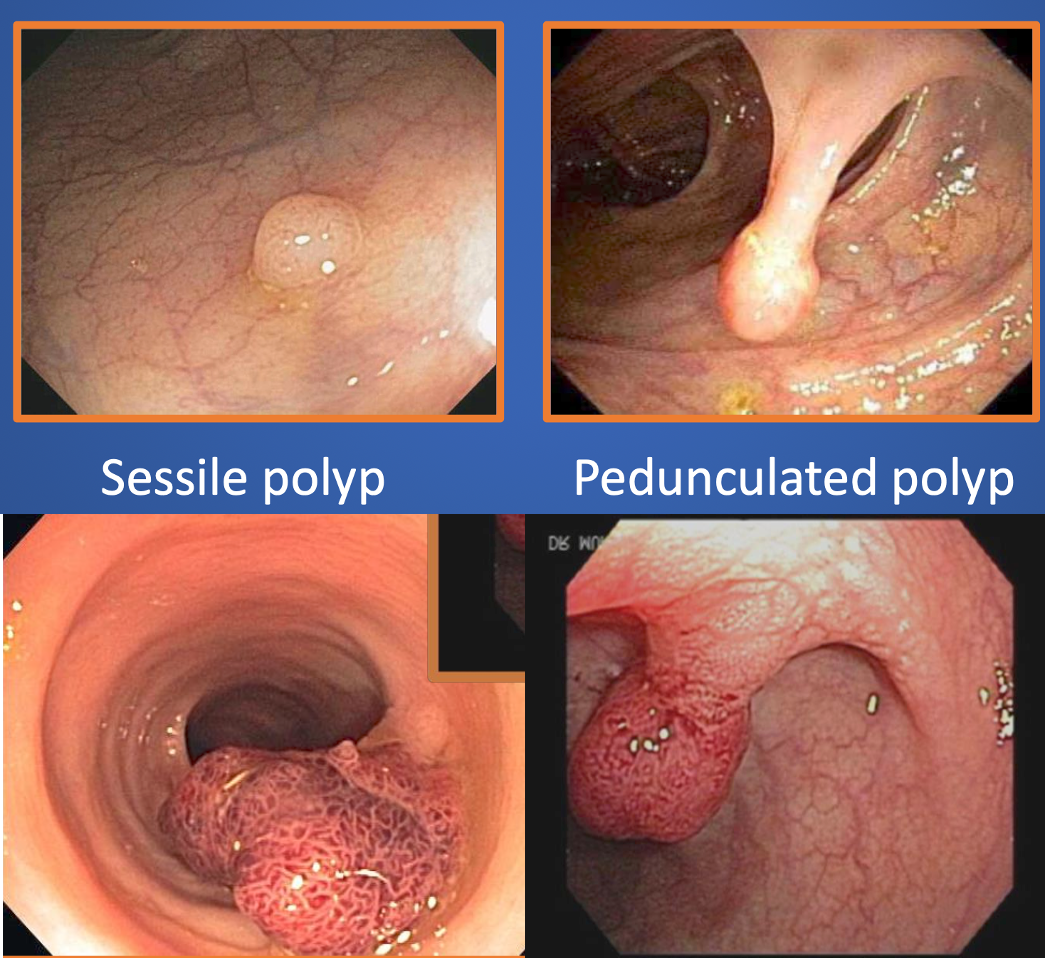
| Attachment | Most often pedunculated | Most often sessile |
Signs and symptoms
- Most patients are asymptomatic.
- Rectal bleeding (Commonest)
- Iron deficiency anemia (Chronic bleeding)
- Diarrhea or constipation, often with decreased stool caliber.
- Massive fluid and electrolyte loss (Villous adenomas of the rectum and distal colon)
- Distal rectal polyps can be detected by digital rectal examination. Otherwise, physical examination findings are typically normal.
Diagnosis
-
Labs: CBC, coagulation, LFT, Renal profile
-
Stool occult blood test
- Detect a proportion (20%-40%) of colonic polyps that are larger than 10 mm in diameter,
-
Flexible sigmoidoscopy
-
Colonoscopy+Bx
-
Capsule endoscopy
Management
Polypectomy:
- Resected once detected
- During colonoscopy
Surgical resection:
- Difficult to remove endoscopically (large, sessile polyps)
- Advanced recurrent colonic polyps
- In the case of (FAP), colon resection remains the only feasible option. * Long-standing ulcerative colitis who have developed high-grade dysplasia or a dysplasia
- Several surgical options should be discussed with the patient, including total colectomy, subtotal colectomy with rectal sparing, and segmental resection.
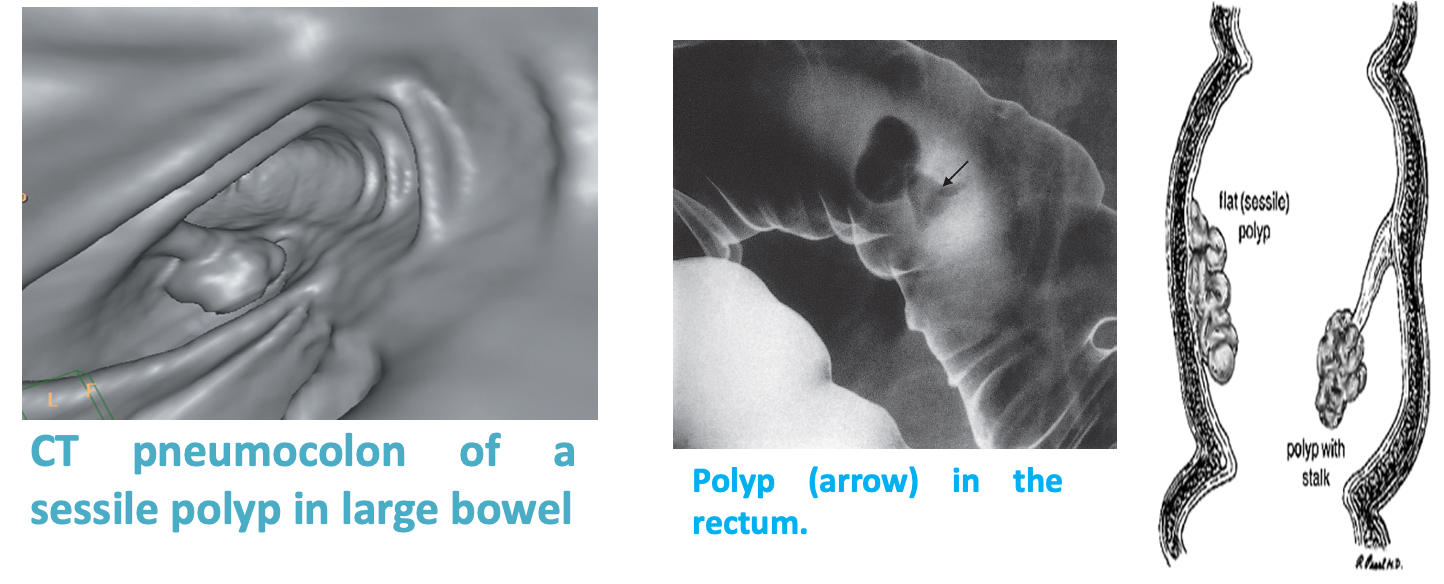
IMAGING
These are mushroom shape fleshy growth on the inner surface of colon. Usually benign but some of these has the potential to malignant transformation.
They are best investigated by endoscopy, but may be found at barium enema or CT pneumocolon.Appear as filling defect on contrast studies